










")








Hirschsprung‘s Disease
Artikel in Produktion, lieferbar vorauss. in 2-3 Wochen
Produktnummer:
MP2079
Artikelnummer: MP2079
Produktinformationen "Hirschsprung‘s Disease"
Clinical History
A 5-year old male presents with a history of constipation since birth. A barium enema showed a constricted rectum with a dilated sigmoid colon. Surgical resection of constricted section of bowl was attempted but the patient died during the surgery.
Pathology
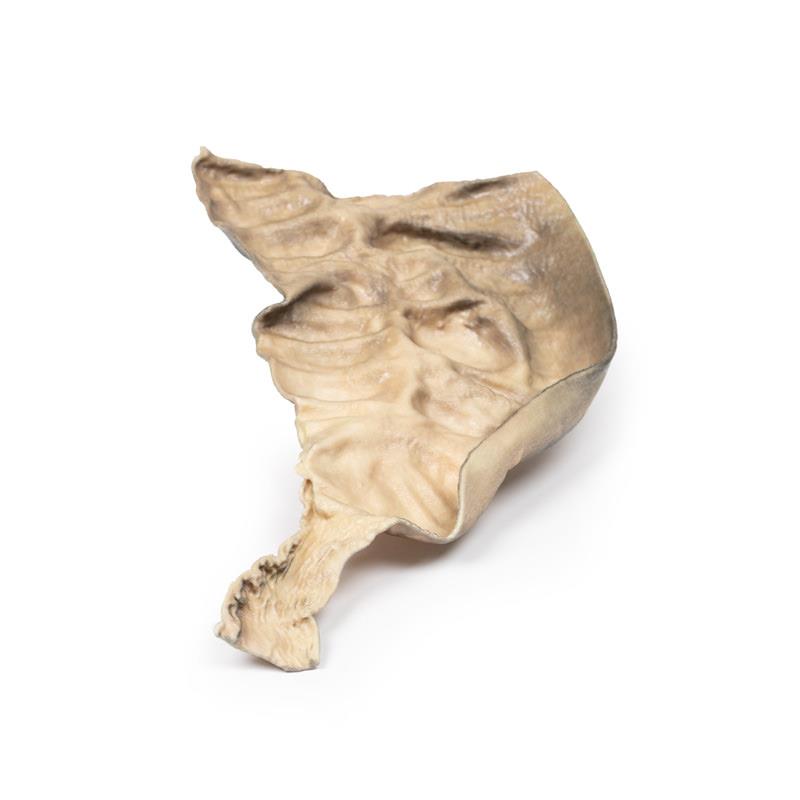
This postmortem section of sigmoid colon has been opened to display the internal surface shown here. There is large dilation of the proximal section of bowel (sigmoid ) with loss of the normal mucosal pattern. The distal section of bowel (rectum) has a normal diameter and a normal mucosal pattern but an absence of ganglion cells in the myenteric plexus. This is an example of Hirschsprung‘s disease, also known as congenital aganglionic megacolon.
Further Information
Hirschsprung‘s disease is characterised by lack of coordinated peristaltic contraction in a segment of bowel, due to a lack of parasympathetic ganglia. It mainly affects the rectum but the length of the aganglionic sections vary. It is caused by defective proximal to distal migration of neural crest cells from the caecum to rectum during embryogenesis, which leads to development of a distal bowel segment lacking both a myenteric and submucosal plexus. This causes an obstruction with hypertrophy and dilation of the proximal normally innervated colon, which can lead to perforation, peritonitis, enterocolitis and electrolyte imbalances.
It occurs in 1 in 5000 live births. It is more common in males, those with siblings with Hirschsprung’s disease and those with other developmental disorders, such as Down Syndrome. Mutations in the receptor tyrosine kinase RET, which is necessary for neural crest cell migration, account for a majority of the familiar cases and 15% of the sporadic cases.
Patients typically present with failure to pass meconium within 48 hours of birth. Less severe cases present later with chronic constipation, vomiting, abdominal pain and distension. Treatment involves resection of the aganglionic section of bowel with anastomosis of the normal sections of bowel to the rectum.
A 5-year old male presents with a history of constipation since birth. A barium enema showed a constricted rectum with a dilated sigmoid colon. Surgical resection of constricted section of bowl was attempted but the patient died during the surgery.
Pathology
This postmortem section of sigmoid colon has been opened to display the internal surface shown here. There is large dilation of the proximal section of bowel (sigmoid ) with loss of the normal mucosal pattern. The distal section of bowel (rectum) has a normal diameter and a normal mucosal pattern but an absence of ganglion cells in the myenteric plexus. This is an example of Hirschsprung‘s disease, also known as congenital aganglionic megacolon.
Further Information
Hirschsprung‘s disease is characterised by lack of coordinated peristaltic contraction in a segment of bowel, due to a lack of parasympathetic ganglia. It mainly affects the rectum but the length of the aganglionic sections vary. It is caused by defective proximal to distal migration of neural crest cells from the caecum to rectum during embryogenesis, which leads to development of a distal bowel segment lacking both a myenteric and submucosal plexus. This causes an obstruction with hypertrophy and dilation of the proximal normally innervated colon, which can lead to perforation, peritonitis, enterocolitis and electrolyte imbalances.
It occurs in 1 in 5000 live births. It is more common in males, those with siblings with Hirschsprung’s disease and those with other developmental disorders, such as Down Syndrome. Mutations in the receptor tyrosine kinase RET, which is necessary for neural crest cell migration, account for a majority of the familiar cases and 15% of the sporadic cases.
Patients typically present with failure to pass meconium within 48 hours of birth. Less severe cases present later with chronic constipation, vomiting, abdominal pain and distension. Treatment involves resection of the aganglionic section of bowel with anastomosis of the normal sections of bowel to the rectum.
Anmelden
Erler-Zimmer
Erler-Zimmer GmbH & Co.KG
Hauptstrasse 27
77886 Lauf
Germany
info@erler-zimmer.de
Achtung! Medizinisches Ausbildungsmaterial, kein Spielzeug. Nicht geeignet für Personen unter 14 Jahren.
Attention! Medical training material, not a toy. Not suitable for persons under 14 years of age.
Andere Kunden kauften auch

Stetige Innovationskraft

Soziale Verantwortung

Gelebte Kundenorientierung

Verständnis für Qualität

Nachhaltiges Handeln

Zertifizierung ISO 9001