










")








Produktinformationen "Ruptured Thoracic Aortic Aneurysm"
Klinische Vorgeschichte
Für dieses Präparat sind keine klinischen Angaben verfügbar.
Pathologie
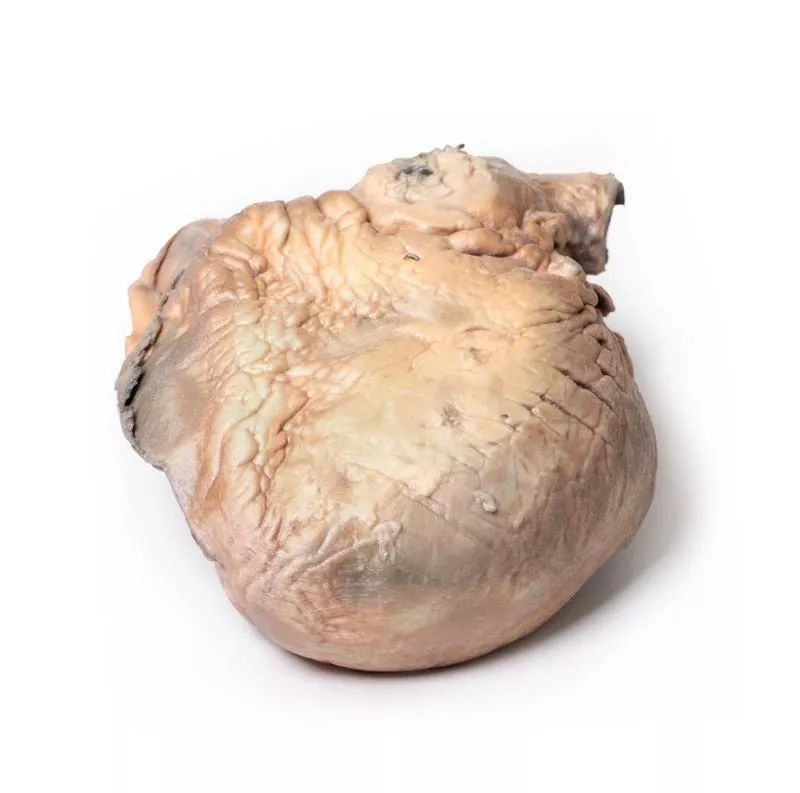
Das Herz wird von der Rückseite gezeigt, beide Ventrikel sind sichtbar. Die aufsteigende thorakale Aorta zeigt eine deutliche sackförmige Erweiterung mit mehreren atherosklerotischen Plaques. Die Aorta ist hinten rupturiert, erkennbar an der dunklen Färbung. Beide Ventrikel sind hypertrophiert, die Koronararterien sowie die Aorten- und Trikuspidalklappen sind normal. Dies stellt ein rupturiertes Aneurysma der aufsteigenden Aorta dar.
Weitere Informationen
Eine Erweiterung der aufsteigenden Aorta wird häufig zufällig bei transthorakaler Echokardiografie entdeckt. Die thorakale Aorta besteht aus drei Abschnitten: aufsteigend, Bogen und absteigend. Die aufsteigende Aorta beginnt direkt oberhalb der Aortenklappe und endet vor dem Brachiocephalicus, ist etwa 5 cm lang. Sie umfasst die Aortenwurzel (mit Koronarsinusen und Sinotubulärem Übergang) und den röhrenförmigen aufsteigenden Abschnitt. Über 50 % der thorakalen Aortenaneurysmen liegen hier und betreffen entweder die Wurzel oder den röhrenförmigen Abschnitt. Ein Aneurysma ist eine örtlich begrenzte Erweiterung der Aorta um mehr als 50 % des erwarteten Durchmessers (Verhältnis beobachtet/erwartet = 1,5) und unterscheidet sich von der Ektasie, einer diffusen Erweiterung unter 50 %. Die Inzidenz der aufsteigenden thorakalen Aortenaneurysmen beträgt etwa 10 pro 100.000 Personenjahre.
Referenz: Saliba et al. (2015). Int J Cardiol Heart Vasc. 6: 91–100.
Für dieses Präparat sind keine klinischen Angaben verfügbar.
Pathologie
Das Herz wird von der Rückseite gezeigt, beide Ventrikel sind sichtbar. Die aufsteigende thorakale Aorta zeigt eine deutliche sackförmige Erweiterung mit mehreren atherosklerotischen Plaques. Die Aorta ist hinten rupturiert, erkennbar an der dunklen Färbung. Beide Ventrikel sind hypertrophiert, die Koronararterien sowie die Aorten- und Trikuspidalklappen sind normal. Dies stellt ein rupturiertes Aneurysma der aufsteigenden Aorta dar.
Weitere Informationen
Eine Erweiterung der aufsteigenden Aorta wird häufig zufällig bei transthorakaler Echokardiografie entdeckt. Die thorakale Aorta besteht aus drei Abschnitten: aufsteigend, Bogen und absteigend. Die aufsteigende Aorta beginnt direkt oberhalb der Aortenklappe und endet vor dem Brachiocephalicus, ist etwa 5 cm lang. Sie umfasst die Aortenwurzel (mit Koronarsinusen und Sinotubulärem Übergang) und den röhrenförmigen aufsteigenden Abschnitt. Über 50 % der thorakalen Aortenaneurysmen liegen hier und betreffen entweder die Wurzel oder den röhrenförmigen Abschnitt. Ein Aneurysma ist eine örtlich begrenzte Erweiterung der Aorta um mehr als 50 % des erwarteten Durchmessers (Verhältnis beobachtet/erwartet = 1,5) und unterscheidet sich von der Ektasie, einer diffusen Erweiterung unter 50 %. Die Inzidenz der aufsteigenden thorakalen Aortenaneurysmen beträgt etwa 10 pro 100.000 Personenjahre.
Referenz: Saliba et al. (2015). Int J Cardiol Heart Vasc. 6: 91–100.
Anmelden
Erler-Zimmer
Erler-Zimmer Medical GmbH
Hauptstrasse 27
77886 Lauf
Germany
info@erler-zimmer.de
Achtung! Medizinisches Ausbildungsmaterial, kein Spielzeug. Nicht geeignet für Personen unter 14 Jahren.
Attention! Medical training material, not a toy. Not suitable for persons under 14 years of age.
Andere Kunden kauften auch

Acute Bacterial Endocarditis
Klinische Vorgeschichte Ein 15-jähriger Junge entwickelte Husten mit Auswurf, gefolgt von hohem Fieber und Brustschmerzen wenige Tage vor Aufnahme im komatösen Zustand. Bei der Untersuchung fiel ein frühes diastolisches Geräusch im Aortenbereich auf, das entlang des linken Brustbeins ausstrahlte. Trotz antibiotischer Therapie verschlechterte sich sein Zustand schnell und er verstarb. Blutkulturen zeigten Staphylococcus aureus.Pathologie Das kleine Herzpräparat zeigt den linken Ventrikel und die zugehörigen Klappen. Die nicht-koronare Klappe der Aortenklappe ist ulzeriert, perforiert und mit brüchigen Vegetationen bedeckt. Unterhalb dieser Klappe erstreckt sich eine Perforation in den rechten Vorhof oberhalb der Trikuspidalklappe. Eine weitere Aortenklappe ist verdickt. Dies ist eine akute bakterielle Endokarditis mit Klappen- und Vorhof-Kammer-Perforationen. Weitere Informationen Akute bakterielle Endokarditis ist eine schwere Infektion der Herzinnenhaut oder Klappen, die meist durch eine vorgeschädigte Endotheloberfläche entsteht. Staphylococcus aureus ist sehr virulent und kann auch gesunde Klappen infizieren. Die Infektion führt zur Aggregation von Thrombozyten und Fibrin, wodurch Vegetationen entstehen, die durch Aktivierung des Gerinnungssystems und Entzündungen wachsen. Diese können embolisieren und Infektionen in anderen Organen verursachen. Risikofaktoren sind Klappenerkrankungen (z. B. rheumatisch oder angeboren), künstliche Klappen oder frühere Herzoperationen. Die Diagnose erfolgt klinisch, durch Blutkulturen und Echokardiografie (transthorakal, transösophageal). Die Behandlung umfasst Antibiotika, Antikoagulanzien und gegebenenfalls chirurgische Eingriffe.

Syphilitic Aneurysm
Klinische Vorgeschichte Ein 61-jähriger Mann stellte sich mit belastungsabhängigem Angina-pectoris-Schmerz und Dyspnoe vor, die sich über 6 Jahre verschlechterten. Bei der Untersuchung zeigte er Zyanose, Tachykardie und einen kollabierenden Puls. Eine Schwellung und ein Pulsationsgeräusch (Thrill) wurden rechts am Hals festgestellt. Der Herzspitzenstoß war inferolateral verlagert. Im Aortenbereich hörte man ein lautes systolisches und diastolisches Geräusch. Das Röntgenbild zeigte eine Kardiomegalie und eine große abgerundete Raumforderung im rechten oberen Mediastinum, die mit dem Herzschatten verbunden war, sowie Hinweise auf Herzversagen. Bluttests waren positiv für Anti-Treponema-Antikörper. Trotz Behandlung verschlechterte sich der Zustand, und der Patient verstarb an Herzversagen.Pathologie Das vergrößerte Herzpräparat umfasst den Aortenbogen und die absteigende Aorta. Die aufsteigende Aorta war bis zu 7 cm erweitert, mit einer großen aneurysmatischen Vorwölbung von 11 x 13 cm. Das Aneurysma wurde geöffnet und zeigte eine runzelige, narbige Intima mit ausgeprägter Atheromatose. Der Brachiocephalicus, die linke gemeinsame Halsschlagader und die Arteria subclavia waren durch das Aneurysma nach links verdrängt. Eine 5 mm hohe, kammartige Verdickung auf der inneren Oberfläche markiert den Ansatz des Perikards. Die kleinen Gefäße der Adventitia zeigten eine starke Stauung. Dies ist ein syphilitisches Aneurysma des Aortenbogens. Weitere Informationen Syphilis ist eine chronische Infektion durch das Bakterium Treponema pallidum, meist sexuell übertragen, gelegentlich auch angeboren. Risikogruppen sind sexuell aktive Personen, intravenöse Drogenkonsumenten, HIV-Patienten und Männer, die Sex mit Männern haben. Penicillin ist die Hauptbehandlung. Syphilis verläuft in drei Stadien: - Primäre Syphilis zeigt sich ca. 3 Wochen nach Infektion mit einem schmerzlosen Ulkus (Schanker), das spontan abheilt. - Sekundäre Syphilis verursacht unspezifische Symptome und Hautausschläge. - Tertiäre Syphilis tritt Jahre später auf und umfasst kardiovaskuläre Syphilis, Neurosyphilis und Gummata.Die kardiovaskuläre Syphilis betrifft die Aortitis der aufsteigenden Aorta mit Erweiterung, Aortenklappeninsuffizienz und Aneurysmen durch Endarteritis der Vasa vasorum. Symptome treten meist 15–30 Jahre nach Infektion auf. Die Neurosyphilis verursacht Kopfschmerzen, Sehverlust, Schlaganfälle und kognitive Störungen. Gummatöse Syphilis zeigt sich durch knotige Läsionen an Haut, Knochen und Schleimhäuten, besonders bei HIV-Patienten.

Traumatic Oesophageal-aortic fistula
Klinische Vorgeschichte Eine Frau verschluckte beim Mittagessen einen Chop-Knochen und brach später zusammen, begleitet von massiver Hämatemesis. Bei der Laparotomie war der Magen mit frischem Blut gefüllt, die Ursache wurde jedoch nicht gefunden. Am Folgetag verstarb sie. Die Autopsie zeigte eine Verbindung zwischen Aorta und Speiseröhre.Pathologie Das Präparat umfasst den distalen Tracheaabschnitt, den Aortenbogen (koronaler Schnitt, von vorne betrachtet) und die Speiseröhre (längs geöffnet). Die Speiseröhren-Schleimhaut ist ulzeriert und blutig. Eine kleine Sonde zeigt eine Fistel zwischen Speiseröhre und der hinteren Wand der thorakalen absteigenden Aorta. Weitere Informationen Obwohl dieser Fall traumatisch verursacht wurde, können aorto-ösophageale Fisteln auch durch nicht-traumatische Ursachen entstehen, etwa durch Druck von Aortenaneurysmen, fortgeschrittene Tumoren oder Erosion von Aortengrafts in den Verdauungstrakt. Diese Fisteln sind lebensbedrohlich und äußern sich meist durch gastrointestinale Blutungen, die von kleinen Blutungen bis zu lebensbedrohlichen Massenblutungen mit Kreislaufversagen reichen. Symptome sind Meläna, offensichtliche Blutungen im Stuhl oder Hämatemesis wie hier. Kleinere Fisteln können auch Unwohlsein oder Durchblutungsstörungen der Beine verursachen. Die Diagnose ist oft schwierig und richtet sich nach Stabilität des Patienten: stabile Patienten werden endoskopisch oder per CT-Angiografie untersucht, instabile benötigen häufig eine sofortige Laparotomie und Bluttransfusionen.

Stetige Innovationskraft

Soziale Verantwortung

Gelebte Kundenorientierung

Verständnis für Qualität

Nachhaltiges Handeln

Zertifizierung ISO 9001