










")






Produktinformationen "Ventriculitis, Secondary to Septicaemia"
Klinische Vorgeschichte
Ein 50-jähriger Alkoholiker wurde mit einer zweiwöchigen Vorgeschichte von Schwäche und Atemnot aufgenommen. Zu Beginn berichtete er über produktiven Husten, Brustschmerzen und blutigen Auswurf. Bei der Untersuchung zeigte er sich fieberhaft, zyanotisch und schläfrig mit pressender Atmung und einem Reibegeräusch über dem rechten Unterlappen. Sein Zustand verschlechterte sich zunehmend. Kurz vor dem Tod wurde eine Lumbalpunktion durchgeführt, wobei grün opaleszierende Flüssigkeit entnommen wurde. Blutkulturen zeigten Streptococcus pneumoniae.
Pathologie
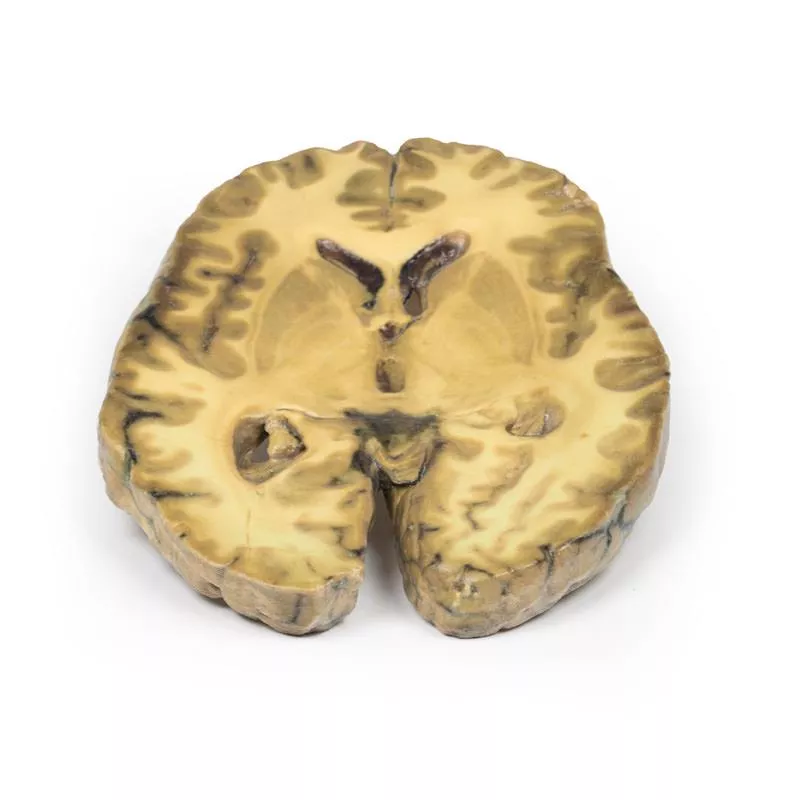
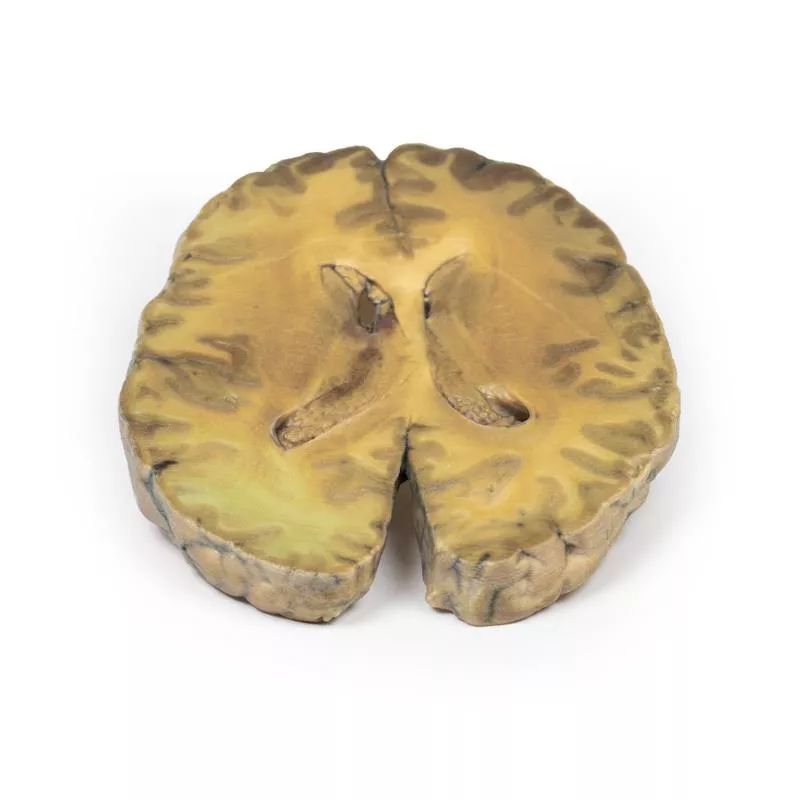
Dieser Fall zeigt eine Ventrikulitis in Kombination mit pneumokokkaler Meningitis und Pneumonie im rechten Basallappen. Ein horizontaler Hirnschnitt zeigt beide Seitenventrikel mit einer verdickten, rauen Ependymschicht und zellulären Ablagerungen nahe dem Choroid plexus und im vorderen Horn. Strukturen wie Caudatus, Lentiformis und innere Kapsel sind erkennbar. Histologisch finden sich massive neutrophile Infiltrationen im Subarachnoidalraum, Gefäßbeteiligung und Entzündungen mit Nekrosen im Gehirnparenchym.
Weitere Informationen
Ventrikulitis ist eine seltene Komplikation intrakranieller Infektionen. Bei Erwachsenen tritt sie meist sekundär nach chirurgischen Eingriffen oder Traumata auf, seltener durch primäre Meningitis. Häufige Erreger sind Staphylokokken und resistente gramnegative Bazillen. Säuglinge unter 6 Monaten sind häufiger betroffen. Symptome ähneln Hydrozephalus bei Aquäduktverschluss. Die Diagnose erfolgt mittels Liquoruntersuchung und Bildgebung (CT, MRT). Die Behandlung erfordert eine langfristige intravenöse Antibiotikatherapie mit guter Liquorgängigkeit.
Ein 50-jähriger Alkoholiker wurde mit einer zweiwöchigen Vorgeschichte von Schwäche und Atemnot aufgenommen. Zu Beginn berichtete er über produktiven Husten, Brustschmerzen und blutigen Auswurf. Bei der Untersuchung zeigte er sich fieberhaft, zyanotisch und schläfrig mit pressender Atmung und einem Reibegeräusch über dem rechten Unterlappen. Sein Zustand verschlechterte sich zunehmend. Kurz vor dem Tod wurde eine Lumbalpunktion durchgeführt, wobei grün opaleszierende Flüssigkeit entnommen wurde. Blutkulturen zeigten Streptococcus pneumoniae.
Pathologie
Dieser Fall zeigt eine Ventrikulitis in Kombination mit pneumokokkaler Meningitis und Pneumonie im rechten Basallappen. Ein horizontaler Hirnschnitt zeigt beide Seitenventrikel mit einer verdickten, rauen Ependymschicht und zellulären Ablagerungen nahe dem Choroid plexus und im vorderen Horn. Strukturen wie Caudatus, Lentiformis und innere Kapsel sind erkennbar. Histologisch finden sich massive neutrophile Infiltrationen im Subarachnoidalraum, Gefäßbeteiligung und Entzündungen mit Nekrosen im Gehirnparenchym.
Weitere Informationen
Ventrikulitis ist eine seltene Komplikation intrakranieller Infektionen. Bei Erwachsenen tritt sie meist sekundär nach chirurgischen Eingriffen oder Traumata auf, seltener durch primäre Meningitis. Häufige Erreger sind Staphylokokken und resistente gramnegative Bazillen. Säuglinge unter 6 Monaten sind häufiger betroffen. Symptome ähneln Hydrozephalus bei Aquäduktverschluss. Die Diagnose erfolgt mittels Liquoruntersuchung und Bildgebung (CT, MRT). Die Behandlung erfordert eine langfristige intravenöse Antibiotikatherapie mit guter Liquorgängigkeit.
Anmelden
Erler-Zimmer
Erler-Zimmer Medical GmbH
Hauptstrasse 27
77886 Lauf
Germany
info@erler-zimmer.de
Achtung! Medizinisches Ausbildungsmaterial, kein Spielzeug. Nicht geeignet für Personen unter 14 Jahren.
Attention! Medical training material, not a toy. Not suitable for persons under 14 years of age.
Andere Kunden kauften auch

Berry Aneurism of Basilar Artery
Klinische VorgeschichteEin 37-jähriger Patient stellte sich mit Kopfschmerzen, Erbrechen und Desorientierung nach einem Kopftrauma vor. Die CT zeigte erweiterte Seitenventrikel und eine in den dritten Ventrikel hineinragende Masse. Aufgrund eines Hydrozephalus wurde ein Shunt gelegt. Die Angiographie ergab ein teilweise thrombosiertes 1 × 1 cm großes Aneurysma der Arteria basilaris. Das Aneurysma vergrößerte sich im Laufe der Zeit, und mehrere chirurgische Versuche, darunter Ligatur und Shunt-Revisionen, blieben erfolglos. Der Patient blieb bewusstlos und verstarb später.PathologieDieser mittlere Sagittalschnitt des Gehirns (1 cm dick) zeigt ein großes, dunkles Beerenaneurysma (5 × 2 cm) aus der Arteria basilaris, das in das Mittelhirn und die Pons eindringt und den dritten Ventrikel komprimiert. Das Aneurysma ist mit einem laminierten Thrombus gefüllt, wobei Blut im dritten Ventrikel sichtbar ist und Anzeichen einer Undichtigkeit vorliegen. In der Pons ist eine mukoide Degeneration (0,4 cm) vorhanden. Die laterale Ansicht zeigt eine Ventrikeldilatation, Blutflecken und einen hämorrhagischen Infarkt des Nucleus caudatus sowie eine meningeale Verfärbung, die mit einer Subarachnoidalblutung vereinbar ist. Weitere InformationenIntrakranielle Aneurysmen treten bei etwa 3,2 % der Bevölkerung auf, mit einer Rupturrate von 7,9 pro 100.000 Personenjahre. Aneurysmen der hinteren Zirkulation sind seltener und treten typischerweise an den Verbindungsstellen der Basilar-, Vertebral- oder Kleinhirnarterien auf. Die Symptome entstehen durch Subarachnoidalblutungen oder Masseneffekte. Zu den Komplikationen zählen erhöhter Hirndruck, Hydrozephalus, erneute Blutungen und Vasospasmen. Zu den Behandlungsoptionen zählen chirurgische und endovaskuläre Eingriffe.

Metastatic Adenocarcinoma in the Brain
Klinische VorgeschichteEin 56-jähriger Mann unterzog sich einer totalen Gastrektomie und Splenektomie aufgrund eines Magenadenokarzinoms. In den folgenden zwei Monaten entwickelte er einen unsicheren Gang, Schwäche der linken Hand sowie frontale Kopfschmerzen mit Übelkeit und Erbrechen. Bildgebung zeigte eine Läsion im rechten Frontallappen. Nach Kraniotomie und Resektion bestätigte sich histologisch ein metastasiertes Magenadenokarzinom. Es kam zu Gelbsucht, Bewusstseinsstörungen und Papillenödem infolge eines erhöhten Hirndrucks. Eine Kontrollbildgebung zeigte ein Rezidiv der Hirnmetastase sowie Lebermetastasen. Der Patient verstarb 9 Monate nach der Gastrektomie.PathologieDer koronale Hirnschnitt zeigt einen umschriebenen, rosagrau marmorierten Tumor im rechten Frontallappen, der sowohl graue als auch weiße Substanz betrifft. Es besteht eine Kompression des rechten Seitenventrikels mit Verlagerung der Mittellinie. Weitere InformationenMagenkrebs zählt weltweit zu den häufigsten krebsbedingten Todesursachen. Risikofaktoren sind männliches Geschlecht, Ernährung, Rauchen und Helicobacter pylori-Infektion. Am häufigsten metastasiert das Adenokarzinom in Leber, Peritoneum, Lunge und Knochen. Hirnmetastasen sind selten (weniger als 1?%) und treten meist im Rahmen einer disseminierten Erkrankung auf. Die Prognose ist schlecht. Die palliative Behandlung umfasst Chirurgie, Strahlentherapie, Steroide, Chemotherapie oder Kombinationen daraus.

Left cerebral infarct
Klinische VorgeschichteDie Patientin war eine 51-jährige Frau, die zwei Jahre vor ihrem Tod einen Schlaganfall erlitten hatte, was zu einer linksseitigen Hemiplegie führte. Bei der Obduktion fanden sich eine ausgeprägte generalisierte Arteriosklerose sowie ein alter Herzinfarkt im linken Ventrikel mit einem parietalen Thrombus.PathologieEin Frontalschnitt des Gehirns zeigt unregelmäßige zystische Hohlräume im Versorgungsgebiet der rechten Arteria cerebri media, typisch für einen älteren Infarkt. Die Wände sind gelblich und teilweise kollabiert. Es liegt eine kompensatorische Erweiterung des linken Seitenventrikels vor. Unterhalb der Corpora mammillaria sind die Arterien moderat arteriosklerotisch, jedoch makroskopisch schwer erkennbar. Weitere InformationenAufgrund der bekannten Herzvorgeschichte mit Thrombusbildung ist anzunehmen, dass der Hirninfarkt durch einen kardialen Thromboembolus verursacht wurde.

Meningioma
Klinische VorgeschichteEine 68-jährige Patientin stellte sich mit neu aufgetretenen epileptischen Anfällen vor und erhielt die Diagnose Epilepsie. In der Anamnese zeigten sich zudem allmähliche Persönlichkeitsveränderungen. Wenige Monate später verstarb sie an einem Herzinfarkt.PathologieDer Tumor befindet sich zwischen den beiden Frontallappen und komprimiert diese. Die Schnittfläche ist rosafarben mit gelblichen Nekroseanteilen. Der Tumor ist vorne mit der Dura mater verbunden. Es handelt sich um ein typisches Beispiel für ein Meningeom. Weitere InformationenMeningeome zählen zu den häufigsten tumornahe Erkrankungen des zentralen Nervensystems, obwohl sie aus Arachnoidalzellen der Hirnhäute (Dura, Arachnoidea, Pia) entstehen, die formal nicht zum ZNS gehören. Sie sind oft mit der Dura oder deren Falten (z.?B. Falx cerebri, Tentorium cerebelli) verbunden und meist gutartig sowie langsam wachsend.Je nach Größe und Lage können Symptome wie Krampfanfälle, Verhaltensänderungen, Sinnesstörungen oder Zeichen eines Hirndrucks auftreten. Viele Meningeome bleiben jedoch asymptomatisch.Die Therapie reicht von Beobachtung über chirurgische Entfernung bis hin zu Strahlentherapie, abhängig vom klinischen Befund.Meningeome sind bei Kindern selten. Das mittlere Erkrankungsalter liegt bei 65 Jahren, Frauen sind häufiger betroffen (3:2). Ionisierende Strahlung, etwa nach Schädelbestrahlung, erhöht das Risiko. Die stärkste genetische Veranlagung besteht bei Neurofibromatose Typ 2 (NF2) – einer autosomal-dominanten Erkrankung durch Mutationen des NF2-Gens auf Chromosom 22, die oft zu multiplen Nerventumoren führt.

Glioma grade 3-4, causing papilloedema
Klinische VorgeschichteDie Patientin, 24 Jahre alt, stellte sich nach einem epileptischen Anfall mit einem auffälligen EEG vor. Sechs Monate später klagte sie über verschwommenes Sehen und Kopfschmerzen. Eine Ophthalmoskopie zeigte beidseitiges Papillenödem, jedoch ohne fokale neurologische Befunde. Bildgebende Verfahren ergaben eine raumfordernde Läsion, die als Gliom Grad III–IV diagnostiziert wurde. Trotz Bestrahlung entwickelte sie kurz darauf eine Schwäche von linkem Arm und Bein. Nach Aufnahme wegen Benommenheit und Erbrechen verstarb sie rasch.PathologieDas Präparat zeigt einen großen intrazerebralen Tumor, der die Seitenventrikel sowie die inneren zwei Drittel der Capsula interna und Basalganglien rechts zerstört. Der Tumor infiltriert über das Corpus callosum und deformiert den Aquädukt. Er ist gut begrenzt, stark vaskularisiert und weist zahlreiche Blutungen und Nekrosen auf, was ihm ein geflecktes Aussehen verleiht.

Cerebral Haemorrhage, secondary to Acute Myeloid Leukaemia
Klinische VorgeschichteEin 22-jähriger Mann stellte sich mit einer zweiwöchigen Vorgeschichte von allgemeinem Unwohlsein, Gewichtsverlust und unerklärlichen Blutergüssen vor. In den Tagen vor der Einweisung entwickelte er Husten mit Auswurf und Fieber. Kurz nach der Aufnahme verlor er plötzlich das Bewusstsein und verstarb wenige Minuten später.PathologieDie horizontale Hirnscheibe zeigt die obere Schnittfläche mit zwei großen Einblutungen im rechten Frontallappen und Parietallappen (je ca. 5 cm) sowie mehreren kleineren Einblutungen in der weißen Substanz beider Hemisphären. Diese Veränderungen entsprechen multiplen intraparenchymalen Hirnblutungen bei einem Patienten mit akuter myeloischer Leukämie (AML). Weitere InformationenSolche Hirnblutungen entstehen durch den Riss kleiner Gefäße und führen häufig zu plötzlichen neurologischen Ausfällen. Bei AML führt die Verdrängung gesunder Blutzellen im Knochenmark zu Thrombozytopenie und erhöhtem Blutungsrisiko. Intrakranielle Blutung ist nach Infektion die zweithäufigste Todesursache bei AML. Auch disseminierte intravasale Gerinnung (DIC) kann auftreten. Die Behandlung richtet sich nach Schweregrad und umfasst ggf. hämatomausräumung, Anfallsbehandlung und Druckmanagement. Die Sterblichkeitsrate ist hoch, insbesondere in den ersten 48 Stunden.

Cerebral Haemorrhage
Klinische VorgeschichteEine 56-jährige Frau wurde nach zwei Episoden schwerer Kopfschmerzen mit Bewusstseinsverlust aufgenommen. Die Untersuchung ergab systemische Hypertonie, Herzvergrößerung und rechtsseitige Hemiparese. Die Angiographie zeigte beidseitige Aneurysmen der mittleren Hirnarterie. Ihr Zustand verschlechterte sich rapide und sie verstarb kurz nach der Aufnahme.PathologieDie parasagittal geschnittene linke Gehirnhälfte zeigt eine große Hirnblutung, die den Parietal- und Frontallappen betrifft. Die Blutung und das damit verbundene Gerinnsel haben die äußere Kapsel und den Seitenventrikel erheblich verformt. Die Blutung ging von einem gerissenen Aneurysma der linken mittleren Hirnarterie aus.

Pituitary Adenoma
Klinische VorgeschichteEin 29-jähriger Mann stellte sich mit einer 22-monatigen Vorgeschichte von Kopfschmerzen und verschwommenem Sehen vor. Es zeigte sich eine bitemporale Hemianopsie sowie eine Parese des VI. Hirnnervs links. Das Schädelröntgen ergab eine Erosion des Keilbeinkörpers, wobei Dorsum sellae und vorderer Processus clinoideus teilweise erhalten waren. Die Karotidenangiographie zeigte eine Aufwärts- und Seitwärtsverlagerung der vorderen und mittleren Hirnarterien. Die Pneumoenzephalographie zeigte eine Verlagerung der Seiten- und dritten Ventrikel nach oben. Nach einer Kraniotomie verstarb der Patient unmittelbar postoperativ.PathologieDie Hypophyse ist vollständig durch einen runden Tumor von 4?cm Durchmesser ersetzt, sichtbar in einem sagittalen Hirnschnitt rechts der Falx cerebri. Die Schnittfläche ist blassbraun und homogen mit einem kleinen hämorrhagischen Areal, vermutlich durch den Eingriff bedingt. Der Tumor führt zu einer Aufwärtsverlagerung des Mittelhirns und zur Zerstörung des Keilbeins, wodurch die Sella turcica erweitert ist. Das Chiasma opticum ist komprimiert. Histologischer Befund: chromophobes Adenom des Hypophysenvorderlappens. Weitere InformationenBei diesem älteren Fall wurden inzwischen veraltete Methoden wie die Pneumoenzephalographie verwendet. Heute wären CT und MRT des Gehirns Standard. Hypophysenadenome sind die häufigsten Hypophysentumoren und treten meist zwischen dem 35. und 60. Lebensjahr auf. Die Symptome ergeben sich aus dem Raumfordernden Effekt – darunter erhöhter Hirndruck, Knochenerosion und Kompression des Chiasma opticum – sowie möglicher hormoneller Aktivität. Etwa 75?% sind funktionell aktiv (z.?B. Prolaktin-, Wachstumshormon- oder ACTH-produzierend). Nicht-funktionelle Tumoren werden meist später entdeckt und können durch Kompression zu Hypopituitarismus führen.

Stetige Innovationskraft

Soziale Verantwortung

Gelebte Kundenorientierung

Verständnis für Qualität

Nachhaltiges Handeln

Zertifizierung ISO 9001