










")












Produktinformationen "Abdomen with bilateral Hernias"
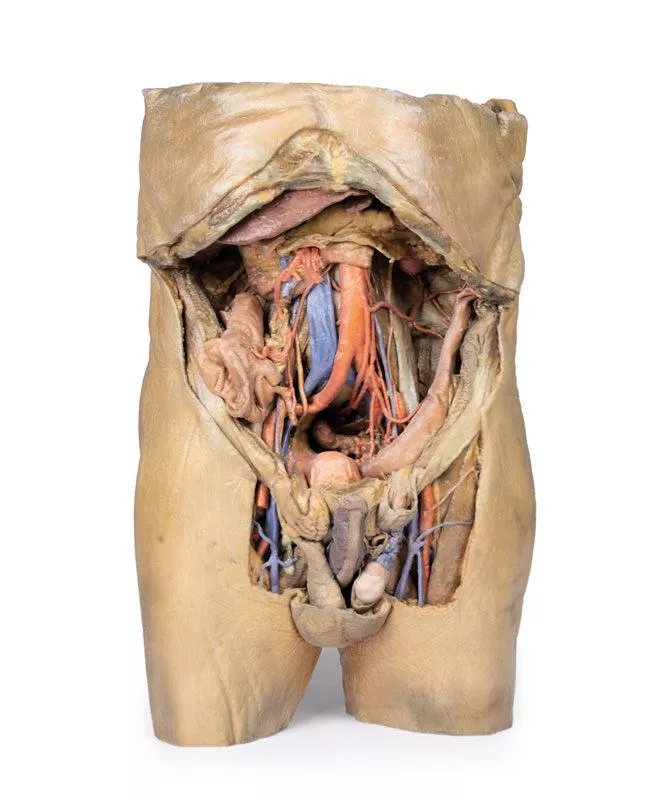
Dieses 3D-Modell ist eines der größten und komplexesten der Serie und besteht aus einem Teil des Rumpfes vom Zwerchfell bis zum proximalen Oberschenkel mit einer vollständigen Bauchhöhle, in der verschiedene Stadien der Dissektion erhalten sind. Dieses 3D-Modell zeigt auch das seltene gleichzeitige Auftreten von indirekten und direkten Leistenbrüchen, wodurch die anatomischen Grundlagen beider Erkrankungen berücksichtigt werden können. Angesichts des Umfangs der Präparation ist die Beschreibung dieses 3D-Modells in einzelne Teile unterteilt, die sich nach Ansichten und Regionen richten.
Das Zwerchfell
Das Zwerchfell ist auf der Oberseite des Modells erhalten geblieben, wobei sowohl die Kuppeln als auch die costodiaphragmatischen Vertiefungen trotz einer gewissen Verzerrung durch die Entfernung der Rippen sichtbar sind. Das fibröse Perikard liegt auf dem zentralen Sehnenstrang, wobei die terminale untere Hohlvene im Foramen cavale zu sehen ist. Seitlich davon liegen die Speiseröhre im Hiatus oesophageus und die absteigende thorakale Aorta, die sich dem Hiatus aorticus in der Nähe der Wirbel nähert.
Die epigastrische und hypochondrische Region
Im Abdomen werden durch die Entfernung der vorderen Wand, des Omentum majus und eines Großteils des Magen-Darm-Trakts die retroperitonealen Strukturen freigelegt. Der terminale Ösophagus mündet links neben der Leber. Nach Entfernung des Magens liegt die Bauchspeicheldrüse von Kopf bis Schwanz vollständig frei und reicht bis zur Milz im linken Hypochondrium. Oberhalb davon überspannen die Milz- und die gemeinsame Leberarterie den engen Raum zwischen Bauchspeicheldrüse, Zwerchfell und Leber. Die gewundene Milzarterie teilt sich in der Nähe der Milzvene; aus der gemeinsamen Leberarterie entspringen die gastroduodenale und die rechte Magenarterie, oberflächlich zur Pfortader. Die oberen Mesenterialgefäße verlaufen in der Nähe des Pankreaskopfes, und die Ileokolische Arterie führt zum Blinddarm. Die Vena mesenterica inferior entspringt aus der Vena rectalis superior und kreuzt die Aorta descendens.
Unterhalb der Leber liegt die Gallenblase zwischen den Lappen. Auf der linken Seite verlaufen die Nierengefäße tief zum Pankreas, wobei die Harnleiter über die Psoas-Muskeln hinabführen.
Die Nabel- und Lendenregion
Die meisten Bauchorgane in der Nabel- und Lendenregion wurden entfernt, um die hintere Bauchwand freizulegen. In der Mitte sind die absteigende Aorta und die untere Hohlvene deutlich zu erkennen, wobei die Hodengefäße bis zur Leistengegend verfolgt werden können. Zwei rechte Lendenarterien zweigen von der Aorta ab, und aus der unteren Mesenterialarterie entspringen die linke Kolikarterie, die Sigmoidarterie und die obere Rektalarterie. Auf der rechten Seite sind die Nerven subcostalis, iliohypogastricus und ilioinguinalis sowie die Arteria circumflexa iliaca sichtbar.
Der Unterbauch und die Beckenregion
Die Bauchaorta verzweigt sich in die Arteria iliaca communis, die Arteria iliaca interna und die Arteria iliaca externa, wobei die entsprechenden Venen iliacae in die Vena cava inferior münden. Die Arteria obturatoria, die Harnleiter und die Hodenarterien sind sichtbar. Im echten Becken bedeckt das Peritoneum die Blase, während das Rektum verdeckt bleibt. Die rechte Fossa iliaca enthält das terminale Ileum, das Caecum und den Appendix mit den nahe gelegenen Gefäßen und Nerven. Auf der linken Seite kreuzt das Sigmoid die Fossa iliaca, wo sich ein Epiploic-Anhang in eine indirekte Hernie in der Nähe der A. epigastrica inferior erstreckt.
Die Leistengegend und der Damm
Dieses Modell zeigt sowohl direkte (rechts) als auch indirekte (links) Leistenhernien, wobei die unteren epigastrischen Gefäße zur anatomischen Orientierung erhalten geblieben sind. Die rechte Hernie liegt medial zu diesen Gefäßen; der linke Bruchsack erstreckt sich lateral in den Samenstrang hinein und enthält einen Epiploonfortsatz. Das Perineum zeigt den Penis, die Hoden und die Samenstränge. Auf der rechten Seite ist der Strang intakt, auf der linken Seite ist er geöffnet und zeigt eine variköse Hodenvene, die mit der indirekten Hernie verbunden ist.
Der Oberschenkel
Das Femurdreieck wurde an beiden Oberschenkeln präpariert. Auf der rechten Seite wurde die Femurscheide entfernt, um die Femoralarterie, die Vene, die tiefen Leistenlymphknoten und den Femoralnerv freizulegen. Auf der linken Seite zeigt eine breitere Ansicht die vorderen und medialen Oberschenkelmuskeln, wobei die Femoralarterie, die Arteria profunda femoris und die Arteria circumflexa iliaca sichtbar sind. Das Modell endet in der Mitte des Oberschenkels und zeigt die Querschnittsanatomie einschließlich des Femurschafts, der Gefäße und der Muskeln im subsartorialen Kanal.
Das Zwerchfell
Das Zwerchfell ist auf der Oberseite des Modells erhalten geblieben, wobei sowohl die Kuppeln als auch die costodiaphragmatischen Vertiefungen trotz einer gewissen Verzerrung durch die Entfernung der Rippen sichtbar sind. Das fibröse Perikard liegt auf dem zentralen Sehnenstrang, wobei die terminale untere Hohlvene im Foramen cavale zu sehen ist. Seitlich davon liegen die Speiseröhre im Hiatus oesophageus und die absteigende thorakale Aorta, die sich dem Hiatus aorticus in der Nähe der Wirbel nähert.
Die epigastrische und hypochondrische Region
Im Abdomen werden durch die Entfernung der vorderen Wand, des Omentum majus und eines Großteils des Magen-Darm-Trakts die retroperitonealen Strukturen freigelegt. Der terminale Ösophagus mündet links neben der Leber. Nach Entfernung des Magens liegt die Bauchspeicheldrüse von Kopf bis Schwanz vollständig frei und reicht bis zur Milz im linken Hypochondrium. Oberhalb davon überspannen die Milz- und die gemeinsame Leberarterie den engen Raum zwischen Bauchspeicheldrüse, Zwerchfell und Leber. Die gewundene Milzarterie teilt sich in der Nähe der Milzvene; aus der gemeinsamen Leberarterie entspringen die gastroduodenale und die rechte Magenarterie, oberflächlich zur Pfortader. Die oberen Mesenterialgefäße verlaufen in der Nähe des Pankreaskopfes, und die Ileokolische Arterie führt zum Blinddarm. Die Vena mesenterica inferior entspringt aus der Vena rectalis superior und kreuzt die Aorta descendens.
Unterhalb der Leber liegt die Gallenblase zwischen den Lappen. Auf der linken Seite verlaufen die Nierengefäße tief zum Pankreas, wobei die Harnleiter über die Psoas-Muskeln hinabführen.
Die Nabel- und Lendenregion
Die meisten Bauchorgane in der Nabel- und Lendenregion wurden entfernt, um die hintere Bauchwand freizulegen. In der Mitte sind die absteigende Aorta und die untere Hohlvene deutlich zu erkennen, wobei die Hodengefäße bis zur Leistengegend verfolgt werden können. Zwei rechte Lendenarterien zweigen von der Aorta ab, und aus der unteren Mesenterialarterie entspringen die linke Kolikarterie, die Sigmoidarterie und die obere Rektalarterie. Auf der rechten Seite sind die Nerven subcostalis, iliohypogastricus und ilioinguinalis sowie die Arteria circumflexa iliaca sichtbar.
Der Unterbauch und die Beckenregion
Die Bauchaorta verzweigt sich in die Arteria iliaca communis, die Arteria iliaca interna und die Arteria iliaca externa, wobei die entsprechenden Venen iliacae in die Vena cava inferior münden. Die Arteria obturatoria, die Harnleiter und die Hodenarterien sind sichtbar. Im echten Becken bedeckt das Peritoneum die Blase, während das Rektum verdeckt bleibt. Die rechte Fossa iliaca enthält das terminale Ileum, das Caecum und den Appendix mit den nahe gelegenen Gefäßen und Nerven. Auf der linken Seite kreuzt das Sigmoid die Fossa iliaca, wo sich ein Epiploic-Anhang in eine indirekte Hernie in der Nähe der A. epigastrica inferior erstreckt.
Die Leistengegend und der Damm
Dieses Modell zeigt sowohl direkte (rechts) als auch indirekte (links) Leistenhernien, wobei die unteren epigastrischen Gefäße zur anatomischen Orientierung erhalten geblieben sind. Die rechte Hernie liegt medial zu diesen Gefäßen; der linke Bruchsack erstreckt sich lateral in den Samenstrang hinein und enthält einen Epiploonfortsatz. Das Perineum zeigt den Penis, die Hoden und die Samenstränge. Auf der rechten Seite ist der Strang intakt, auf der linken Seite ist er geöffnet und zeigt eine variköse Hodenvene, die mit der indirekten Hernie verbunden ist.
Der Oberschenkel
Das Femurdreieck wurde an beiden Oberschenkeln präpariert. Auf der rechten Seite wurde die Femurscheide entfernt, um die Femoralarterie, die Vene, die tiefen Leistenlymphknoten und den Femoralnerv freizulegen. Auf der linken Seite zeigt eine breitere Ansicht die vorderen und medialen Oberschenkelmuskeln, wobei die Femoralarterie, die Arteria profunda femoris und die Arteria circumflexa iliaca sichtbar sind. Das Modell endet in der Mitte des Oberschenkels und zeigt die Querschnittsanatomie einschließlich des Femurschafts, der Gefäße und der Muskeln im subsartorialen Kanal.
Anmelden
🔬 3D-Anatomie-Reihe – Nachbildungen des menschlichen Körpers!
26. August 2025
Entdecken Sie exklusive 3D-gedruckte Modelle des menschlichen Körpers – aus echten Präparaten erstellt.
Erler-Zimmer
Erler-Zimmer Medical GmbH
Hauptstrasse 27
77886 Lauf
Germany
info@erler-zimmer.de
Achtung! Medizinisches Ausbildungsmaterial, kein Spielzeug. Nicht geeignet für Personen unter 14 Jahren.
Attention! Medical training material, not a toy. Not suitable for persons under 14 years of age.
Andere Kunden kauften auch

Female hemipelvis and thigh
Dieses detaillierte 3D-Modell zeigt die linke Hälfte eines weiblichen Beckens, das in der mittleren Sagittalebene geschnitten ist und sich bis zur proximalen Mitte des Oberschenkels erstreckt.Beckenorgane und Peritoneum- Sichtbare Strukturen: Harnblase, Gebärmutter, Scheide und Enddarm (von vorne nach hinten).- Das Peritoneum ist erhalten und zeigt die vesikouterinen und rektouterinen Taschen.- Das breite Ligament, der Eileiter, die Fimbrien und der linke Eierstock sind in der Nähe des Beckenrandes erkennbar. Gefäße und Nerven- Die A. iliaca communis und die A. iliaca externa verlaufen neben der V. iliaca communis und dem M. psoas major in Richtung des subinguinalen Raums.- Der Ureter kreuzt diese Gefäße.- Der N. femoralis ist zwischen dem M. psoas major und dem M. iliacus sichtbar. Vorderer Oberschenkel und Leistenbereich- Die oberflächliche Faszie wurde entfernt, wodurch die Strukturen des Oberschenkels bis zum Rand des Perineums freigelegt wurden.- Das Femurdreieck wurde präpariert, um Folgendes zu zeigen:- Die Arteria femoralis und die Vena femoralis, wobei die Vene Zuflüsse aus der Vena saphena magna, der Vena circumflexa iliaca superficialis, der Vena pudenda externa und der Vena pudenda profunda erhält.- Der Nervus femoralis lateral zur Arterie.- Die vorderen Hautnerven und ein Teil des lateralen Hautnervs über dem Sartorius-Muskel.- Die Leistenlymphknoten unterhalb des Leistenbandes. Hintere Gesäßregion- Der große Gesäßmuskel wurde entfernt, um die tiefer liegenden Gesäßmuskeln freizulegen.- Der Piriformis-Muskel wurde zurückgezogen, wodurch Folgendes freigelegt wurde:- Der Ischiasnerv, der aus dem Nervus tibialis und dem Nervus peroneus communis gebildet wird.- Die Arteria glutea superior und inferior.- Der N. cutaneus posterior femoris verläuft parallel zum Ischiasnerv.- Die Muskeln M. obturatorius internus, M. gemelli und M. quadratus femoris werden freigelegt.- Die A. pudenda interna und der N. pudendus verlaufen in Richtung Fossa ischioanalis.- Ihre Äste, darunter der N. rectalis inferior, sind in der Nähe des Beckenzwerchfells und des äußeren Analsphinkters sichtbar.

Abdomen vasculature
Coeliacus-StammDer Coeliacus-Stamm entspringt auf Höhe von T12 und versorgt den embryonalen Vorderdarm. Zu den sichtbaren Ästen gehören die linke Magenarterie auf der linken Seite, die Milzarterie, die zum linken Hypochondrium verläuft, und die gemeinsame Leberarterie auf der rechten Seite. Aus der gemeinsamen Leberarterie entspringen die gastroduodenale Arterie, die mit der A. mesenterica superior verbunden ist, und die eigentliche Leberarterie, die sich in die linke und rechte Leberarterie verzweigt. Die rechte Leberarterie bildet schließlich die Arteria cystica, die die Gallenblase versorgt. A. mesenterica superior und A. mesenterica inferiorDie A. mesenterica superior und die A. mesenterica inferior entspringen an L1 und L3 und versorgen den Mitteldarm und den Hinterdarm. Obwohl sie nicht vollständig erhalten ist, ist die A. mesenterica superior unterhalb der Bauchspeicheldrüse sichtbar und verzweigt sich, während die A. mesenterica inferior entlang der linken Seite der Aorta verläuft. Die A. colica sinistra verzweigt sich von der A. mesenterica inferior und versorgt den Dickdarm über die Arteriae marginale. Venensystem des AbdomensDie Vena mesenterica superior liegt posterior zur Arterie und erscheint weniger röhrenförmig. Durch die Entfernung des linken Leberlappens werden die Äste der Pfortader freigelegt, die Nährstoffe aus dem Darm zu den Hepatozyten transportieren, bevor sie über die Lebervenen in die Vena cava inferior abfließen.Hilum der NiereDie rechte Niere weist eine typische Anatomie auf, mit der Nierenvene oben, der Arterie unten und dem Harnleiter nach unten verlaufend. Die linke Niere weist Abweichungen auf: Die Nierenvene ist unten und unterteilt, die Arterie ist oben und der Harnleiter verläuft nach medial. Muskeln, Nerven und andere GefäßeDer Musculus psoas major und der Musculus iliacus sind auf beiden Seiten sichtbar, umgeben von wichtigen Nerven des Plexus lumbalis – insbesondere auf der linken Seite –, darunter der Nervus iliohypogastricus, der Nervus ilioinguinalis, der Nervus femoralis und der Nervus genitofemoralis. Medial zum Musculus psoas major sind die linke Hodenarterie (aus der Aorta) und die Vene (die in die linke Nierenvene mündet) zu sehen. Die rechte Hodenvene mündet direkt in die IVC. Ein Ast der Arteria iliolumbalis verläuft unterhalb der Hodengefäße und des Ureters. GallenblaseUnmittelbar unterhalb der Leber ist die Gallenblase zu sehen, zu der die Arteria cystica nach unten verläuft. Der Ductus cysticus ist ebenfalls zu sehen, der von der Gallenblase ausgeht und sich mit dem Ductus hepaticus aus der Leber verbindet, um den Ductus choledochus zu bilden.

Spleen and pancreas
Dieses detaillierte anatomische 3D-Modell zeigt die tief liegenden Organe des Vorderdarms, darunter den absteigenden, horizontalen und aufsteigenden Teil des Zwölffingerdarms, die Bauchspeicheldrüse und die Milz. Es bietet einen einzigartigen und aufschlussreichen Einblick in die komplexe Anatomie dieser Region. ZwölffingerdarmIm Zwölffingerdarm ist ein kleines Fenster geöffnet, um die Plicae circularis, die charakteristischen kreisförmigen Falten des proximalen Dünndarms, sichtbar zu machen. Dies steht im Kontrast zu den markanten Falten des Magens und ermöglicht einen lehrreichen Vergleich der Schleimhautmuster im oberen Magen-Darm-Trakt. BauchspeicheldrüseDie Bauchspeicheldrüse ist in ihrer natürlichen anatomischen Position erhalten, eingebettet in die Krümmung des Zwölffingerdarms. Der Kopf der Bauchspeicheldrüse ist deutlich sichtbar, einschließlich des ausgeprägten Uncus an seinem distalen Rand, der an den Ursprung der A. mesenterica superior (SMA) angrenzt. In diesem Modell ist die SMA bereits in ihre wichtigsten benannten Äste unterteilt, wodurch ihre vaskuläre Komplexität hervorgehoben wird.Der Körper der Bauchspeicheldrüse weist den oberen Rand auf, an dem sich der aus der absteigenden Bauchaorta abgezweigte Truncus coeliacus befindet. Die gesamte Milzarterie ist mit ihrem gewundenen Verlauf vom Truncus coeliacus zur Milz dargestellt. Das Modell zeigt auch die Ursprünge der linken Magenarterie und der gemeinsamen Leberarterie, die vom Truncus coeliacus abzweigen.Angrenzend an den Truncus coeliacus ist ein Abschnitt der Milzvene zu sehen, der aus der Pankreaskapsel austritt. Diese Vene verläuft entlang der Milzarterie auf ihrem Weg zur Milz. Zusätzlich ist ein Teil der Vena mesenterica superior zu sehen, der an der hinteren Bauchspeicheldrüse anliegt und ihren Verlauf darstellt, bevor sie mit der Milzvene zusammenfließt, um die Pfortader zu bilden.Der Schwanz der Bauchspeicheldrüse ist in die Milzkapsel eingebettet und verdeckt teilweise die Äste der Milzarterie, bevor diese in die Milz eintritt. Für detailliertere Ansichten dieser Region verweisen wir auf unsere anderen Milzmodelle (MP1130 und MP1134), die weitere anatomische und räumliche Zusammenhänge veranschaulichen.

Female pelvis deep dissection
Dieses hochdetaillierte 3D-Modell zeigt eine tiefgehende Präparation des weiblichen Beckens, isoliert von den umgebenden Regionen, mit Schwerpunkt auf den viszeralen, vaskulären und ligamentären Strukturen in Bezug auf knöcherne Orientierungspunkte.Beckenorgane und peritoneale Strukturen- Der Sigmoidkolon verläuft über den Beckenrand hinunter in das Rektum und kreuzt dabei die gemeinsamen und äußeren Beckenarterien.- In der Nähe befinden sich die Sigmoid- und die obere Rektalarterie sowie der absteigende Harnleiter.- Die Harnblase (kollabiert) und die Gebärmutter befinden sich anterior im eigentlichen Becken.- Das breite Ligament ist erhalten, während die Eierstöcke, Eileiter, Eierstock- und Rundbänder zwar vorhanden, aber aufgrund altersbedingter Atrophie undeutlich sind.- Das Aufhängeband und das Rundband sind vom Peritoneum abgelöst, um die umgebenden Gefäße freizulegen. Arterien und Venen- Die Äste der A. iliaca interna sind beidseitig sichtbar.- Die A. sacralis mediana ist in der Mittellinie zwischen den A. iliaca communis zu sehen.- Linke Seite: Nur A. uterina.- Rechte Seite: A. uterina, A. vesicalis superior und A. obturatoria.- Die A. epigastrica inferior und die V. epigastrica inferior entspringen aus den A. iliaca externa und sind in der Nähe der unteren Bauchwand sichtbar. Muskuloskelettale Merkmale- Rechte Seite: Der gesamte Femur und die Oberschenkelmuskulatur wurden entfernt, um Folgendes freizulegen:- Obturatormembran- Acetabularknorpel- Transversales Acetabulargelenkband- Die posteriore Dissektion zeigt:- Foramen gluteum superium und Arteria glutea superior- Ligamentum sacrospinale (mit entferntem Ligamentum sacrotuberale)- Die untere Rektalarterie verzweigt sich innerhalb der Fossa ischioanalis. Nerven und Bänder- Der linke Ischiasnerv ist innerhalb des Foramen ischiadicum magnum erhalten geblieben.- Das Ligamentum sacrotuberale ist auf der linken Seite erhalten geblieben.- Die Fossae ischioanalis auf beiden Seiten zeigen:- Verzweigungen der unteren Rektalarterie- Fasern des Beckenmembran- Integration des äußeren Analsphinkters mit der Rektumwand

Vasculature of the spleen
Dieses anatomische Modell zeigt anschaulich das Milzhilum und konzentriert sich dabei auf die wichtigen Gefäßstrukturen, die die Milz versorgen und entwässern.Hauptmerkmale:Milzarterie und -vene:Beide Gefäße treten am Hilum in die Milz ein. Die Öffnung der Milzvene wird durch einen eingesetzten Silikonschlauch offen gehalten, sodass die venöse Drainage deutlich sichtbar ist. Das Modell zeigt den obersten Ast der Milzvene, der sorgfältig durchtrennt wurde, um seinen Verlauf sichtbar zu machen. Gewundene Milzarterie:Das Modell hebt die charakteristische gewundene und gekräuselte Form der Milzarterie hervor, die sich am Hilum verzweigt und ihren natürlichen, gewundenen Verlauf vom Truncus coeliacus zur Milz widerspiegelt. Verzweigte Gefäße:Aus der Milzarterie und -vene gehen die kurzen Magenarterien und die linke Magen-Omentum-Arterie hervor. In diesem Präparat sind diese Äste über ihren Ursprung hinaus durchtrennt, sodass sie nicht vollständig sichtbar sind und ein fokussierter Blick auf die Hauptgefäße am Hilum ermöglicht wird.Bänderverbindungen (nicht vorhanden):- Splenorenales Band: Verbindet die Milz mit der linken Niere und enthält die Milzarterie, die Milzvene und den Pankreasschwanz. Dieses Band, das embryologisch aus dem Peritoneum des dorsalen Mesenteriums gebildet wird, wurde im Modell entfernt, um die Milzgefäße deutlich sichtbar zu machen.- Gastrosplenisches Ligament: Verbindet den Magen mit der Milz und enthält die kurzen Magenarterien und einen Teil der linken Magen-Omentum-Arterie. Dieses Ligament fehlt ebenfalls im Modell, da die Präparation über den Milzarterienast hinausgeht. Milzkapsel:Die Außenfläche der Milz ist von einer dünnen fibrösen Kapsel bedeckt. Diese empfindliche Schicht neigt aufgrund des hohen Blutgehalts der Milz zu Rupturen, was eine wichtige klinische Überlegung ist, die durch das Modell hervorgehoben wird.

Abdomen with inguinal hernia
Zwerchfell und XiphoidfortsatzDas Zwerchfell wurde mit Nähten am oberen Rand des präparierten Präparats befestigt, um eine ungehinderte Sicht auf den Bauchraum zu gewährleisten. Der Xiphoidfortsatz befindet sich in der Mitte dieses genähten Randes. Leber und GallenblaseDie Leber im rechten Hypochondrium wird seitlich verschoben, um die dahinter liegende Niere freizulegen. Das Ligamentum falciforme dividit dividiert den rechten und linken Leberlappen und enthält das Ligamentum teres, einen Rest der fetalen Nabelvene. Unterhalb des Ligamentum teres liegt die Gallenblase zwischen den Leberlappen. Magen und MilzgefäßeDer entleerte Magen wird nach oben geschoben, um die verdrehte Milzarterie und -vene freizulegen, die sich in den Milzhilus verzweigen.Milz und BauchspeicheldrüseDie Milz befindet sich im linken Hypochondrium, wobei ihre Magenabdruck die große Kurvatur des Magens markiert. Der Schwanz der Bauchspeicheldrüse, der intraperitoneal ist und mit dem Milzhilus verwachsen ist, liegt in der Nähe ihres unteren Pols. NierenDie Nieren liegen größtenteils retroperitoneal, aber das sie bedeckende Peritoneum wurde bei diesem Präparat entfernt. Normalerweise liegt die rechte Niere aufgrund der Leber tiefer, aber hier ist sie kleiner und liegt höher als die linke. Die linke Niere ist vergrößert, mit zwei zusätzlichen Nierenarterien aus der Aorta, die ihr Hilum und ihren unteren Pol versorgen.NebennierenDie linke Nebenniere ist von ihrer üblichen Position am oberen Pol der Niere abgelöst. Die mittlere Nebennierenarterie entspringt direkt aus der Aorta links vom Truncus coeliacus, während die untere Nebennierenarterie aus der linken Nierenarterie abzweigt: Beide versorgen die Nebenniere. Die obere Nebennierenarterie ist durch Bindegewebe verdeckt.Rektum und BlaseObwohl der größte Teil des Peritoneums im Abdomen unterhalb der Höhe des Sakralfortsatzes (S1) entfernt wurde, bleibt eine Schicht des Peritoneums intakt, die das Rektum und die Blase überlagert. Bemerkenswert ist, dass dies der erste Teil des Rektums ist, der intraperitoneal liegt. Magen-Darm-TraktDer letzte Teil des aufsteigenden Zwölffingerdarms und der absteigende Dickdarm an der linken Kolikflexur wurden mit einer Schnur ligiert, wobei der dazwischen liegende Darm entfernt wurde, um eine bessere Sicht auf den Bauchraum zu ermöglichen. BeckenregionBei diesem Präparat ist das Sigmoid indirekt durch den Leistenkanal herniert. Auf der rechten Seite tritt der Samenleiter aus dem oberflächlichen Leistenring in Richtung des rechten Hodens aus, während andere Inhalte des Samenstrangs entfernt wurden. Nähte unterhalb des Samenleiters markieren den Einstich für die Einbalsamierung über die rechte Oberschenkelarterie.BauchgefäßeDer Truncus coeliacus, der sich direkt unterhalb des Magens befindet, verzweigt sich typischerweise in die linke Magenarterie, die Milzarterie und die gemeinsame Leberarterie, um den Vorderdarm zu versorgen.In diesem 3D-Modell entspringen aus dem Truncus coeliacus die rechte und linke Magenarterie, die Milzarterie und ein gastroduodenaler Ast, der sich in zwei obere Pankreas-Duodenal-Arterien aufteilt. Die rechte Leberarterie entspringt unabhängig von der Bauchaorta und gibt die rechte untere Zwerchfellarterie ab. Die Arteria iliolumbalis entspringt tief zum rechten Psoas und verbindet sich mit Ästen der rechten tiefen Arteria circumflexa iliaca entlang des Beckenkamms.

Stomach
This 3D model is an isolated stomach with two dissection windows to expose the rugae and pylorus. A small portion of the terminal oesophagus is preserved at the cardiac region, and a small portion of the proximal duodenum beyond the pyloric sphincter. The large window within the body of the stomach allows for a clear view into the fundus and the well-developed rugae on the posterior aspect of the wall of the organ. The smaller window, opened just at the pyloric region, allows for an appreciation of the thickening of the organ wall at the pyloric sphincter just proximal to the start of the duodenum.

Internal abdominal wall
Dieses detaillierte 3D-Modell zeigt die innere Oberfläche der vorderen Bauchwand – ein Bereich, der bei Präparationen häufig entfernt oder beschädigt wird. Es ergänzt unser MP1130-Bauchpräparat, bei dem die vordere Wand entfernt wurde, und bietet einen klaren Blick auf wichtige Muskel- und Bindegewebsstrukturen.Hauptmerkmale:Muskelfasern und Aponeurose:Die horizontal ausgerichteten Muskelfasern des Musculus transversus abdominis laufen zu ihrer Aponeurose (Sehnenblatt) zusammen, die insbesondere entlang der oberen Ränder des Präparats sichtbar ist. Arcuate Line:Diese Landmarke befindet sich im unteren Drittel des Modells und markiert die Stelle, an der sich die Aponeurose relativ zum Musculus rectus abdominis verschiebt.- Oberhalb der Arcuate Line: Die Aponeurosefasern teilen sich gleichmäßig um den Musculus rectus abdominis.- Unterhalb der bogenförmigen Linie: Alle Aponeurosefasern verlaufen anterior zum Musculus rectus abdominis, was eine Veränderung der Bauchwandstruktur widerspiegelt. Gefäßstrukturen:Arterien und Venen der unteren Epigastriumregion:Diese Gefäße entspringen aus den Arterien und Venen der A. iliaca externa und verlaufen superior durch die vordere Bauchwand. Hesselbach-Dreieck:Auf der rechten Seite des Modells definiert die Ausrichtung der unteren epigastrischen Arterie relativ zum Musculus rectus abdominis den Scheitelpunkt des Leisten- (Hesselbach-) Dreiecks – einer kritischen anatomischen Region, die häufig mit direkten Leistenbrüchen in Verbindung gebracht wird. (Hinweis: Das Leistenband, das die Basis dieses Dreiecks bildet, ist in diesem Präparat nicht vorhanden.) Embryologischer Rest: Medianes Bauchband:Diese Falte des parietalen Peritoneums befindet sich in der Mittellinie zwischen den beiden geraden Bauchmuskeln und bedeckt den Urachus, einen fibrösen Rest aus der embryonalen Entwicklung, der sich von der Blase bis zum Nabel erstreckt.

Male hemipelvis and thigh
Dieses 3D-Modell zeigt einen rechten männlichen Beckenabschnitt, der knapp oberhalb des L5-Wirbels und in der mittleren Sagittalebene geschnitten wurde, wobei der Oberschenkel bis nahe an den mittleren Schaft des Femurs erhalten geblieben ist. Dieses Präparat ergänzt unser LW 91-Präparat des weiblichen Hemipelvis und Oberschenkels. Die A. iliaca communis ist erhalten, wobei mehrere wichtige Äste sichtbar sind, insbesondere die Verteilung der A. iliaca interna innerhalb des echten Beckens. Mehrere große Gefäße, darunter die Arteria obturatoria und die teilweise obliterierte Arteria umbilicalis, verlaufen in Richtung der vorderen Bauchwand (um das Ligamentum umbilicale mediale zu bilden) und geben die Arteria vesicalis superior ab, während die Wurzeln der Arteria iliolumbalis, Arteria glutea superior, Arteria glutea inferior und Arteria pudenda interna lateral zur Harnblase sichtbar sind. Der Harnleiter verläuft oberflächlich zu diesen Gefäßen hinab zur Harnblase, die in diesem Modell mit Peritoneum bedeckt ist. Der Ductus deferens ist vom Eintritt in den Raum über den tiefen Leistenring bis zum hinteren Verlauf freigelegt (obwohl er von seinem normalen Einmündungsweg abgeschnitten ist und auf der A. iliaca interna aufliegt). Angrenzend an den Harnleiter und an der oberflächlichen Oberfläche des Musculus psoas major befindet sich ein vergrößerter Lendenlymphknoten und ein Teil des Lymphgefäßsystems, das entlang der Arteria iliaca externa aufsteigt. Der größte Teil des Beckens wurde nicht präpariert, sodass die Rektovesikale Tasche und die freigelegte Arteria rectalis superior und Vena rectalis, die sich dem erhaltenen Teil des Rektums nähern, gut zu erkennen sind. Im Querschnitt sind das Rektum, die Samenblase und die Prostata sichtbar (die Schnittebene bewahrt Teile sowohl der prostatischen Harnröhre als auch des Ejakulationskanals).Im vorderen Oberschenkelbereich sind die Grenzen und Inhalte des Femurdreiecks gut erhalten und teilweise durch den Lappen der vorderen Bauchwand bedeckt. Posterior wurden die Haut über der Gesäßregion und der Musculus gluteus maximus als sequenzielle Fenster entfernt, um den Musculus gluteus medius und minimus, den Musculus piriformis, den Musculus obturatorius internus mit den Musculi gemelli und den Musculus quadratus femoris freizulegen. Die Arteria glutea superior und inferior bleiben oberhalb bzw. unterhalb des Musculus piriformis erhalten, wobei der Nervus ischiadicus unterhalb des Musculus piriformis austritt, bevor er tief unter dem erhaltenen Teil des Musculus gluteus maximus verläuft.

Liver with vessels and gallbladder
Dieses Leberpräparat weist im Vergleich zu einer typischen Leber deutliche Unterschiede auf. Es ist weniger keilförmig und in der superoinferioren Dimension verlängert, was zu einer größeren vertikalen Höhe führt, wenn man es von hinten betrachtet. Größe: - Misst entlang der mittleren Klavikularlinie etwa 18 cm.- Typische Lebern messen in dieser Dimension weniger als 16 cm.- Die erhöhte Länge deutet auf eine leichte Hepatomegalie (Vergrößerung) hin. Wichtige Hinweise:- Größenschätzungen können durch die Konservierung und Fixierung der Probe beeinflusst werden, was zu Verzerrungen führen kann.- Die Diagnose einer Hepatomegalie auf der Grundlage einer einzigen Messung ist begrenzt und variiert je nach individueller Anatomie, Messtechnik, Geschlecht und Body-Mass-Index (BMI). Anatomische Variationen:Diese Probe entspricht nicht den üblichen anatomischen Variationen, die häufig mit einer Hepatomegalie verwechselt werden, wie z. B.:- Riedel-Lappen: eine nach unten gerichtete Ausstülpung des rechten Lappens- Biber-Schwanz-Leber: verlängerter linker Lappen- Papillärer Fortsatz des Caudatus-Lappens

Stetige Innovationskraft

Soziale Verantwortung

Gelebte Kundenorientierung

Verständnis für Qualität

Nachhaltiges Handeln

Zertifizierung ISO 9001