










")






Produktinformationen "Glioblastoma multiforme"
Klinische Vorgeschichte
Über einen Zeitraum von 3 Jahren litt eine 57-jährige Frau an intermittierenden Stirnkopfschmerzen und Gedächtnisstörungen, die sich zu psychiatrischen Symptomen, Erbrechen und Meningismus entwickelten. Lokal neurologische Ausfälle traten erst spät auf.
Pathologie
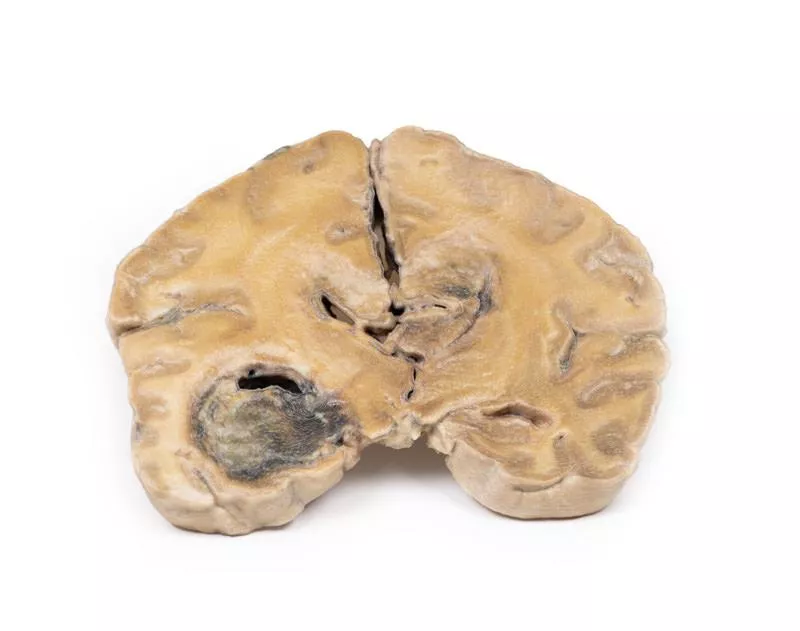
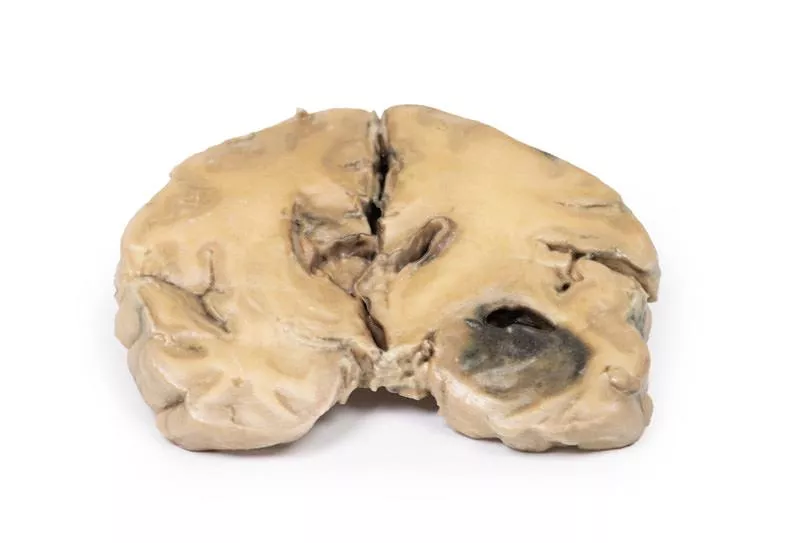
In koronaren Hirnschnitten zeigt sich ein runde, hämorrhagische und unterschiedlich gefärbte Tumor im linken Temporallappen. Das Tumorgewebe erstreckt sich über die Mittellinie und ersetzt den Corpus callosum. Das Ventrikelsystem ist nahezu komplett obliteriert. Weitere Schnitte bestätigten, dass es sich um einen einzigen großen Tumor handelt.
Weitere Informationen
Gliome sind nach Meningeomen die zweithäufigsten Tumoren des ZNS. Sie ähneln histologisch normalen Makrogliazellen wie Astrozyten, Oligodendrozyten und Ependymzellen und entstehen aus entsprechenden Vorläuferzellen. Das Glioblastom multiforme (GBM), ein Grad IV Astrozytom, kann de novo oder aus niedriggradigen Gliomen entstehen. Charakteristisch sind Nekrosen, umgeben von anaplastischen Zellen und hyperplastischen Gefäßen. GBMs treten häufiger bei Männern auf und werden meist im 6. Lebensjahrzehnt diagnostiziert. Risikofaktoren sind Neurofibromatose Typ 1, Li-Fraumeni-Syndrom und frühere Hirnstrahlentherapie. Symptome variieren je nach Lage und umfassen Kopfschmerzen, Sehstörungen, Erbrechen, Appetitverlust, Stimmungsschwankungen, kognitive Veränderungen, neu aufgetretene Anfälle und Sprachstörungen. Diagnostisch werden CT und MRT eingesetzt. Etwa 50 % der GBMs betreffen mehr als eine Hemisphäre, infiltrieren oft Ventrikelwände oder Hirnhäute und erreichen gelegentlich den Liquor. Metastasen außerhalb des ZNS sind selten. Das Tumorwachstum führt zu Hirnödem und erhöhtem Hirndruck. Ohne Behandlung beträgt die mittlere Überlebenszeit etwa 3 Monate. Die Therapie besteht aus Operation, Strahlen- und Chemotherapie.
Über einen Zeitraum von 3 Jahren litt eine 57-jährige Frau an intermittierenden Stirnkopfschmerzen und Gedächtnisstörungen, die sich zu psychiatrischen Symptomen, Erbrechen und Meningismus entwickelten. Lokal neurologische Ausfälle traten erst spät auf.
Pathologie
In koronaren Hirnschnitten zeigt sich ein runde, hämorrhagische und unterschiedlich gefärbte Tumor im linken Temporallappen. Das Tumorgewebe erstreckt sich über die Mittellinie und ersetzt den Corpus callosum. Das Ventrikelsystem ist nahezu komplett obliteriert. Weitere Schnitte bestätigten, dass es sich um einen einzigen großen Tumor handelt.
Weitere Informationen
Gliome sind nach Meningeomen die zweithäufigsten Tumoren des ZNS. Sie ähneln histologisch normalen Makrogliazellen wie Astrozyten, Oligodendrozyten und Ependymzellen und entstehen aus entsprechenden Vorläuferzellen. Das Glioblastom multiforme (GBM), ein Grad IV Astrozytom, kann de novo oder aus niedriggradigen Gliomen entstehen. Charakteristisch sind Nekrosen, umgeben von anaplastischen Zellen und hyperplastischen Gefäßen. GBMs treten häufiger bei Männern auf und werden meist im 6. Lebensjahrzehnt diagnostiziert. Risikofaktoren sind Neurofibromatose Typ 1, Li-Fraumeni-Syndrom und frühere Hirnstrahlentherapie. Symptome variieren je nach Lage und umfassen Kopfschmerzen, Sehstörungen, Erbrechen, Appetitverlust, Stimmungsschwankungen, kognitive Veränderungen, neu aufgetretene Anfälle und Sprachstörungen. Diagnostisch werden CT und MRT eingesetzt. Etwa 50 % der GBMs betreffen mehr als eine Hemisphäre, infiltrieren oft Ventrikelwände oder Hirnhäute und erreichen gelegentlich den Liquor. Metastasen außerhalb des ZNS sind selten. Das Tumorwachstum führt zu Hirnödem und erhöhtem Hirndruck. Ohne Behandlung beträgt die mittlere Überlebenszeit etwa 3 Monate. Die Therapie besteht aus Operation, Strahlen- und Chemotherapie.
Anmelden
Erler-Zimmer
Erler-Zimmer Medical GmbH
Hauptstrasse 27
77886 Lauf
Germany
info@erler-zimmer.de
Achtung! Medizinisches Ausbildungsmaterial, kein Spielzeug. Nicht geeignet für Personen unter 14 Jahren.
Attention! Medical training material, not a toy. Not suitable for persons under 14 years of age.
Andere Kunden kauften auch

Intracranial space-occupying lesion
Klinische Vorgeschichte Eine 56-jährige Frau wurde nach einer Grand-Mal-Epilepsie bewusstlos ins Krankenhaus eingeliefert. Sie hatte zuvor über einen Zeitraum von sechs Monaten an wiederkehrenden Kopfschmerzen und Erbrechen gelitten. Das Bewusstsein erlangte sie nicht mehr zurück.Pathologie In der koronaren Schnittfläche des Gehirns zeigt sich eine seitliche und nach unten gerichtete Verdrängung durch eine große, vermutlich rechtsseitige meningeale Raumforderung. Die eigentliche Raumforderung (wahrscheinlich ein Meningeom) ist nicht erhalten. An der Vorderseite zeigt sich eine Mittellinienverlagerung mit subfalkiner Herniation des Gyrus cinguli. Auf der Rückseite finden sich Blutungen unterschiedlicher Altersstufen im Temporallappen und Brückenbereich (Pons), typisch für supratentorielle Raumforderungen. Zusätzlich ist eine Ventrikelasymmetrie sichtbar. Weitere InformationenEin Meningeom mit raumfordernder Wirkung kann Druck auf das Hirngewebe ausüben, was zu Atrophie und Verlagerung führt und die Funktion von Hirnnerven, die Blutzirkulation und die normalen Gehirnfunktionen beeinträchtigen kann. Häufige Symptome sind: - Krampfanfälle – z.?B. myoklonisch (Muskelzuckungen oder Spasmen) oder tonisch-klonisch (Bewusstlosigkeit, Muskelsteifigkeit, gefolgt von Zuckungen, Kontrollverlust über Körperfunktionen). - Sinnesstörungen – Veränderungen des Seh-, Geruchs- oder Hörsinns ohne Bewusstseinsverlust.Die Symptomatik hängt stark von der Lokalisation des Tumors ab.

Astrocytoma
Klinische VorgeschichteEine 73-jährige Frau wurde mit neu aufgetretener linksseitiger Hemiplegie stationär aufgenommen. In der Anamnese klagte sie über eine drei Monate bestehende Kombination aus Kopfschmerzen, Übelkeit und zunehmender Unsicherheit beim Gehen. Die CT zeigte einen inoperablen Hirntumor. Sie verstarb eine Woche nach Aufnahme.Pathologie Ein koronar geschnittenes Gehirn zeigt einen unscharf begrenzten Tumor im rechten Temporallappen, begleitet von hemisphereller Erweiterung und glätten der Windungen. Die Rückansicht offenbart eine subfalkine Herniation, und der Tumor weist Bereiche mit Nekrose und Blutung auf. Die Histologie bestätigen ein Astrozytom Grad III/IV. Weitere InformationenAls Teil der Gliome – der zweithäufigsten Hirntumorgruppe nach Meningeom – entstehen Astrozytome aus Astrozyten. Gestaffelt nach Grad: diffus (II), anaplastisch (III) bis Glioblastom (IV). Histologisch typisch: Gemistocyten mit eosinophiler Zytoplasma-Kontrastiert mit fibrillärem Hintergrund. Am häufigsten in den Hemisphären bei Patienten im Alter von 40–60 Jahren. Klinisch treten Anfälle, Kopfschmerzen, Übelkeit und neurologische Defizite auf. Ohne Therapie liegt das mittlere Überleben bei Grad III bei etwa 18 Monaten. Therapiert wird mit OP, Strahlentherapie, Chemotherapie oder sinnvoller Kombination.

Metastatic carcinoma in the brain
Klinische VorgeschichteDiese 51-jährige Frau hatte zwei Jahre vor ihrer Vorstellung eine Operation wegen eines Mammakarzinoms hinter sich. Sie klagte über linksseitige Ataxie, die seit zwei Wochen bestand. Zuvor war es zu einer Ohnmacht mit nachfolgender Schwäche der linken Seite gekommen. Die Untersuchung ergab eine spastische Parese links. Aufgrund des raschen Symptombeginns wurde zunächst eine vaskuläre Ursache vermutet. Nach Entlassung aus dem Krankenhaus wurde sie sechs Wochen später wegen linksseitiger Krampfanfälle erneut aufgenommen. Lumbalpunktion und Re-Untersuchung brachten keine klaren Ergebnisse. Das EEG zeigte eine rechts temporale Störung, und die Angiographie bestätigte eine raumfordernde Läsion im rechten Großhirn. Ihr Zustand verschlechterte sich kontinuierlich und führte schließlich zum Tod.PathologieDie horizontale Schnittfläche des Gehirns zeigt drei zystische Tumoren, hauptsächlich im rechten Parietallappen. Der größte misst 5 cm im Durchmesser, ein weiterer liegt nahe dem hinteren Rand des größten Tumors, und ein dritter befindet sich im linken Parietallappen. Die Tumoren betreffen vorwiegend die weiße Substanz und weisen eine zerklüftete, graue Wand auf. Der größte Tumor hatte in den rechten Seitenventrikel ulzeriert. Es lag eine subfalkine Herniation mit Verlagerung der Basalganglien und Kapsula interna vor. Die Histologie bestätigte ein metastasiertes Karzinom. Weitere Metastasen fanden sich in Leber und Knochen, was mit einem primären Mammakarzinom vereinbar ist.

Glioblastoma multiforme
Klinische VorgeschichteEin 56-jähriger Mann stellte sich nach einem generaliserten Krampfanfall vor, blieb bewusstlos und verstarb später. Die Anamnese ergab sechs Monate fortschreitende Verwirrung, Kurzzeitgedächtnisverlust und Persönlichkeitsveränderungen.PathologiePostmortale koronare Hirnschnitte zeigen einen 4 cm großen nekrotischen und hämorrhagischen Tumor, der vom unteren Frontallappen in den Seitenventrikel einwächst. Auf der Rückseite ist eine meningeale Ausbreitung sichtbar. Weitere InformationenGliome sind nach Meningeomen die zweithäufigsten Tumoren des Zentralnervensystems. Sie stammen von gliazellähnlichen Zellen wie Astrozyten, Oligodendrozyten oder Ependymzellen ab. Das Glioblastom multiforme (GBM), ein Grad-IV-Astrozytom, entwickelt sich aus Astrozyten und kann de novo oder aus niedriggradigen Tumoren entstehen. Histologisch zeigen GBMs Nekrose, umgeben von anaplastischen Zellen und hyperplastischen Blutgefäßen. Männer sind häufiger betroffen, meist im 6. Lebensjahrzehnt. Risikofaktoren sind Neurofibromatose Typ 1, Li-Fraumeni-Syndrom und frühere Hirnstrahlentherapie. Symptome richten sich nach Lokalisation und umfassen anhaltende Kopfschmerzen, Sehstörungen, Erbrechen, Appetitverlust, Stimmungsschwankungen, kognitive Verschlechterung, Krampfanfälle und Sprachstörungen. Diagnostik erfolgt mittels CT und MRT. Rund 50 % der GBMs befallen mehr als eine Hemisphäre und infiltrieren oft Ventrikel oder Hirnhäute, eine Ausbreitung ins Rückenmark ist selten. Metastasen außerhalb des ZNS sind ungewöhnlich. Das Tumorwachstum führt zu Hirnödem und erhöhtem Hirndruck. Diese aggressiven Tumoren haben unbehandelt eine Überlebenszeit von etwa 3 Monaten. Die Behandlung umfasst Operation, gefolgt von Strahlen- und Chemotherapie.

Metastatic melanoma
Klinische VorgeschichteIn den 1970er Jahren stellte sich eine 31-jährige Frau mit starken Kopfschmerzen und Doppeltsehen vor, acht Monate nach der Entfernung eines invasiven pigmentierten Hautmelanoms am Hals. Bei der Erstuntersuchung wurden keine Auffälligkeiten festgestellt. Nach Entlassung wurde sie wegen anhaltendem Erbrechen erneut aufgenommen. Ihr Zustand verschlechterte sich rasch und sie verstarb kurz darauf.PathologieDas Hirnpräparat zeigt ausgedehnte Melanommetastasen. Auf der unteren Oberfläche finden sich zahlreiche dunkle Knoten von bis zu 1,5 cm Durchmesser. Auch auf der oberen Schnittfläche sind ähnliche Läsionen sichtbar, die ausschließlich in der grauen Substanz liegen. Die Tumorherde sind nicht kapsuliert, infiltrieren die Hirnrinde und zeigen Nekrosen und Einblutungen. Weitere InformationenEtwa 10 % aller Hirnmetastasen stammen von Melanomen. Risikofaktoren sind Alter über 60 Jahre, männliches Geschlecht, Krankheitsstadium sowie genetische Mutationen wie BRAF oder NRAS. Die meisten Metastasen sind supratentoriell lokalisiert und können sich mit Kopfschmerzen, neurologischen Ausfällen oder Krampfanfällen äußern. Spontane Blutungen sind möglich. Die Diagnose erfolgt mittels Bildgebung und Histologie. Behandelt wird häufig mit stereotaktischer Radiochirurgie, Radiotherapie sowie Immun- oder zielgerichteter Therapie, was die mittlere Überlebenszeit auf ca. 11 Monate erhöht hat.

Ruptured Berry Aneurysm
Klinische Vorgeschichte Fünf Tage vor der Aufnahme verspürte eine 38-jährige Frau plötzlich Schmerzen hinter dem rechten Auge, gefolgt von einer zunehmenden Schwäche im linken Bein. Bei der Untersuchung zeigte sie sich verwirrt und hypertensiv, mit linksseitiger Hemiparese, rechtsseitiger homonymer Hemianopsie sowie einer VI. Hirnnervenlähmung rechts. Es bestand Kloni an Knie und Sprunggelenk links und ein pathologischer Babinski-Reflex. Die Lumbalpunktion ergab einen erhöhten Druck und blutgetränkte Liquorflüssigkeit. Die Angiographie zeigte ein zerebrales Aneurysma, das operativ geklippt wurde. Am Tag nach der Operation verstarb die Patientin plötzlich.Pathologie Auf der basalen Hirnfläche zeigt sich ein 5 mm großes sakkuläres Aneurysma an der Verbindung der rechten A. carotis interna mit der A. communicans posterior, das rupturiert ist. Es liegt ein Subarachnoidalblutung im Bereich der Cisterna magna und auf der Unterseite des rechten Frontallappens vor. Auf der linken Seite befindet sich ein ähnliches, nicht rupturiertes Aneurysma. Der rechte Frontallappen wirkt weich und brüchig. Weitere Informationen Aneurysmen der A. communicans posterior sind die dritthäufigsten im Circulus arteriosus Willisii und können benachbarte Hirnnerven wie den VI. Hirnnerv komprimieren. Die Augenschmerzen lassen sich durch Reizung des Trigeminusnervs erklären. Das Sichtfelddefizit resultiert wahrscheinlich aus Druck auf das rechte Sehbahnsegment. Die neurologischen Symptome richten sich nach dem betroffenen Versorgungsgebiet der Hirnrinde.

Cerebral Arterio-Venous Malformation
Klinische VorgeschichteDer 58-jährige Patient verstarb an postoperativen Komplikationen nach einer transurethralen Resektion der Prostata. Bereits mit 28 und 35 Jahren hatte er vorübergehende neurologische Ausfälle. Mit 50 entwickelte er eine permanente Hemiparese des linken Beins, insbesondere im Bereich des Sprunggelenks.PathologieDie koronale Hirnscheibe durch die Parietallappen zeigt eine 4 cm große Läsion in der medialen rechten Hemisphäre, die sich vom Kortex bis zur Seitenventrikeldecke erstreckt. Das Gewebe besteht aus einem Netzwerk geschlängelter Gefäßkanäle. Histologisch wurde eine arteriovenöse Malformation (AVM) mit glialem Gewebe und dilatierten Arterien und Venen bestätigt. Weitere InformationenZerebrale AVMs können Symptome wie Kopfschmerzen, Krampfanfälle und Hirnnervenausfälle verursachen, bleiben aber manchmal unbemerkt. Bei einem Gefäßriss kann es zu Hirnblutungen kommen mit Symptomen wie Bewusstlosigkeit, Übelkeit, Erbrechen und Sehstörungen. Je nach Ort der Blutung sind einseitige Lähmungen (Hemiparese) oder Sprachstörungen (Aphasie) möglich. Rupturierte AVMs gehen mit hoher Sterblichkeit und Langzeitfolgen einher.

Craniopharyngioma
Klinische VorgeschichteEine 62-jährige Frau stellte sich mit Desorientierung bezüglich Zeit, Ort und Person vor. Die körperliche Untersuchung zeigte keine lokalen neurologischen Ausfälle. Bildgebende Verfahren zeigten eine raumfordernde Läsion im Boden des 3. Ventrikels. Bei der Operation wurde Gewebe entfernt, eine vollständige Entfernung war jedoch nicht möglich. Die Histologie bestätigte die Diagnose eines Kraniopharyngeom. Postoperativ entwickelten sich komplexe metabolische Störungen, vermutlich hypothalamisch bedingt. Der Zustand der Patientin verschlechterte sich zunehmend und sie verstarb 10 Wochen nach Aufnahme nach einer Magenaspiration.PathologieDas sagittal geschnittene Gehirn zeigt einen rosa-grauen, ovalen Tumor von 2,5 x 1,5 cm Größe in der Hypothalamusregion. Der Tumor ist kapsuliert, außer an der ventralen Seite, wo bei der Operation Gewebe entfernt wurde. Die Schnittfläche zeigt ein mikrozystisches oder schwammartiges Erscheinungsbild. Der Tumor verformt den 3. Ventrikel und verlegt das Foramen Monroi. Der Chiasma opticum ist nach unten verlagert. Ein früherer Ventrikulo-atrialer Shunt verhinderte trotz der Verlegung die Erweiterung der Seitenventrikel. Weitere InformationenKraniopharyngeome machen 1–3 % aller Hirntumore aus und 5–10 % der Hirntumore bei Kindern. Die Erkrankung zeigt eine bimodale Altersverteilung mit Häufigkeitsgipfeln zwischen 5–14 und 50–75 Jahren. Die Inzidenz ist in Japan und Teilen Afrikas höher. Es handelt sich um epitheliale Tumoren, die meist vom Hypophysenstiel ausgehen, aber auch aus der Sella turcica, dem optischen System oder dem 3. Ventrikel stammen können. Sie bestehen häufig aus festen und zystischen Anteilen, letztere enthalten Cholesterinkristalle. Es gibt zwei Haupttypen: das adamantinomatöse und das papilläre Kraniopharyngeom, die sich histologisch und genetisch unterscheiden, wobei die Prognoseunterschiede unklar sind. Die Behandlung umfasst operative Resektion und Strahlentherapie zur Behandlung von Resttumor. Die Prognose hängt von der Tumorkontrolle sowie lokalen und endokrinen Komplikationen ab.

Intracerebral Haemorrhage
Klinische Vorgeschichte Ein 80-jähriger Mann verlor plötzlich das Bewusstsein. Bei der Untersuchung zeigten sich eine Blickparese nach rechts, eine linksseitige Hemiplegie und eine rechtsseitige Hemiparese.Pathologie Koronarschnitte auf Höhe der Mamillarkörper, mit Hirnstamm und vorderen Temporallappen, zeigen ein massives Hämatom, das das Gewebe in den linken Basalganglien und der Capsula interna ersetzt. Die Blutung rupturierte in den linken Seitenventrikel und dessen temporalen Horn, zerstörte die Wand und infiltrierte benachbartes Hirngewebe. Auch der rechte Seitenventrikel ist mit Blut gefüllt, besitzt jedoch intakte Wände. Das Hämatom wirkt raumfordernd, dehnt die linke Hemisphäre und verlagert die Mittellinie nach rechts. Eine erkennbare subfalkine Herniation des linken Gyrus cinguli unterhalb der Falx cerebri ist vorhanden. Weitere Informationen Diese Form der intrazerebralen Blutung entsteht meist durch systemische Hypertonie. Sie entsteht durch Ruptur eines Mikroaneurysmas von Ästen der Striatalarterien, die die Basalganglien versorgen.

Stetige Innovationskraft

Soziale Verantwortung

Gelebte Kundenorientierung

Verständnis für Qualität

Nachhaltiges Handeln

Zertifizierung ISO 9001