


















Product information "Abdominal Aortic Aneurysm"
Clinical History
This 70-year-old man with a history of mild gastro-oesophageal reflux suddenly developed severe upper abdominal pain radiating to the left shoulder tip. On examination, he was distressed and hyperventilating, with a pulse rate of 87/min and blood pressure 140/90 mmHg. Abdominal exam showed board-like rigidity and reduced bowel sounds. Emergency laparotomy revealed no ruptured viscus; the pancreas appeared normal, but an unruptured abdominal aortic aneurysm was noted. Endoscopy the next day identified a ruptured oesophageal ulcer, and a Celestin tube was placed. Despite treatment, he developed localized infection, pulmonary oedema, and congestion, dying 19 days after admission.
Pathology
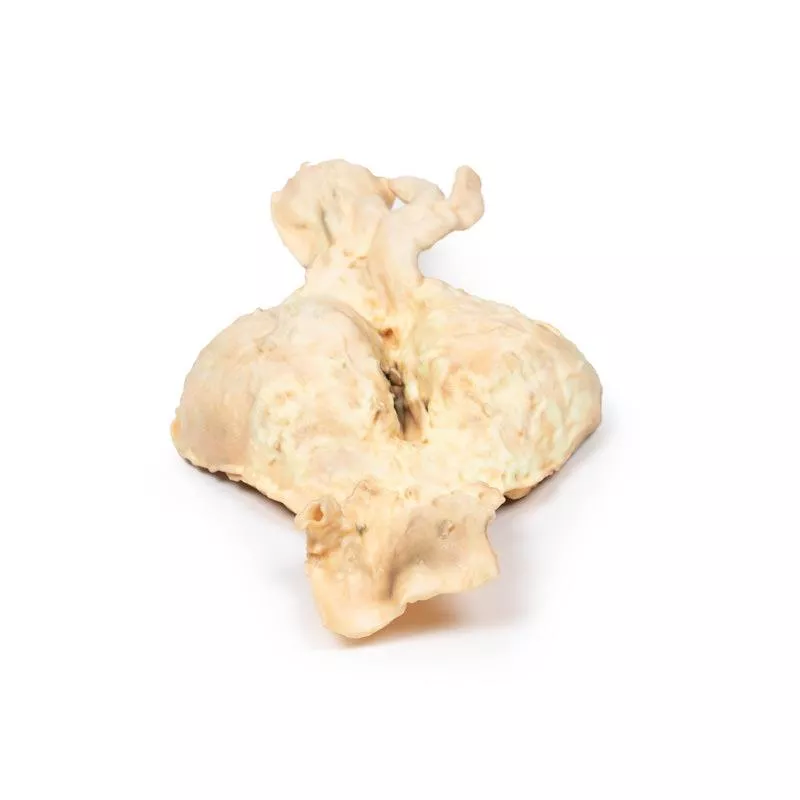
The specimen shows the lower abdominal aorta, common iliac vessels, and proximal iliac arteries. A large 10 x 7 cm aneurysm lies below the renal arteries, extending to the aortic bifurcation. The aneurysm wall is severely thinned and partly lined by laminated thrombus, indicating chronicity. Recent thrombus formation is also evident. There is aneurysmal dilatation of the common iliac and left external iliac arteries. Multiple focally ulcerated atheromatous plaques are present at the upper aorta. No rupture is seen.
Further Information
An abdominal aortic aneurysm (AAA) is a localized enlargement of the abdominal aorta (diameter >3 cm or >50% larger than normal). Most AAAs are asymptomatic unless ruptured. Large aneurysms may be palpable, and sometimes abdominal, back, or leg pain occurs. Rupture causes sudden abdominal/back pain, low blood pressure, unconsciousness, and often death. AAAs mainly affect men over 50, especially smokers or those with high blood pressure or family history. Genetic conditions like Marfan’s and Ehlers-Danlos syndromes also increase risk. About 85% of AAAs occur below the kidneys, making them the most common aortic aneurysm.
This 70-year-old man with a history of mild gastro-oesophageal reflux suddenly developed severe upper abdominal pain radiating to the left shoulder tip. On examination, he was distressed and hyperventilating, with a pulse rate of 87/min and blood pressure 140/90 mmHg. Abdominal exam showed board-like rigidity and reduced bowel sounds. Emergency laparotomy revealed no ruptured viscus; the pancreas appeared normal, but an unruptured abdominal aortic aneurysm was noted. Endoscopy the next day identified a ruptured oesophageal ulcer, and a Celestin tube was placed. Despite treatment, he developed localized infection, pulmonary oedema, and congestion, dying 19 days after admission.
Pathology
The specimen shows the lower abdominal aorta, common iliac vessels, and proximal iliac arteries. A large 10 x 7 cm aneurysm lies below the renal arteries, extending to the aortic bifurcation. The aneurysm wall is severely thinned and partly lined by laminated thrombus, indicating chronicity. Recent thrombus formation is also evident. There is aneurysmal dilatation of the common iliac and left external iliac arteries. Multiple focally ulcerated atheromatous plaques are present at the upper aorta. No rupture is seen.
Further Information
An abdominal aortic aneurysm (AAA) is a localized enlargement of the abdominal aorta (diameter >3 cm or >50% larger than normal). Most AAAs are asymptomatic unless ruptured. Large aneurysms may be palpable, and sometimes abdominal, back, or leg pain occurs. Rupture causes sudden abdominal/back pain, low blood pressure, unconsciousness, and often death. AAAs mainly affect men over 50, especially smokers or those with high blood pressure or family history. Genetic conditions like Marfan’s and Ehlers-Danlos syndromes also increase risk. About 85% of AAAs occur below the kidneys, making them the most common aortic aneurysm.
Login
Erler-Zimmer
Erler-Zimmer Medical GmbH
Hauptstrasse 27
77886 Lauf
Germany
info@erler-zimmer.de
Achtung! Medizinisches Ausbildungsmaterial, kein Spielzeug. Nicht geeignet für Personen unter 14 Jahren.
Attention! Medical training material, not a toy. Not suitable for persons under 14 years of age.
Other customers also bought

Congenital Pulmonary Stenosis
Clinical History This male child had a cardiac murmur detected at birth but remained well until 10 months of age. In the two weeks before hospital admission, he became lethargic, developed a mild cough, and experienced rapid weight gain. Swelling of the face, hands, and feet developed 10 days before admission. On examination, he appeared chubby, with a blood pressure of 90/59 mmHg. A fine thrill was present over the entire precordium, and a harsh systolic murmur was loudest in the pulmonary area. Peripheral oedema was noted. Despite treatment, his condition worsened, and death occurred due to congestive cardiac failure.Pathology The specimen is the child’s heart, viewed from the left. The pulmonary artery has been opened to show the upper surface of the pulmonary valve, which is malformed into a thickened conical diaphragm with a tiny 2 mm opening at the apex. A large post-stenotic dilatation of the pulmonary artery is visible. There is marked right-sided cardiac enlargement, with dilatation of the right atrium and auricle, as well as right ventricular hypertrophy. This case represents an example of pure pulmonary valve stenosis.Further Information Pulmonary stenosis accounts for approximately 7% of congenital heart defects. It can be isolated or part of more complex conditions like Tetralogy of Fallot. The severity of pulmonary stenosis ranges from mild to severe. While mild forms may remain undiagnosed for years, moderate stenosis may progress and severe cases cause substantial strain on the heart, leading to right ventricular hypertrophy and cardiac failure. Complications may include infective endocarditis and arrhythmias due to structural heart changes. Diagnosis is commonly made via echocardiography, though MRI and CT are also used. Surgical correction is now routinely possible.

Rheumatic endocarditis
Clinical HistoryA 52-year-old woman presented with increasing dyspnoea. Her history included childhood fever with migratory joint pains following a sore throat. On examination, she was cyanotic, in atrial fibrillation, had elevated jugular venous pressure, a pan-systolic murmur at the apex, hepatomegaly, and dependent oedema. She received digoxin, furosemide, and penicillin but died after cardiac arrest.Pathology The opened heart shows the left atrium and ventricle. The mitral valve is thickened. The left atrial wall is lined with blood and fibrin, and the appendage is filled with clot due to atrial fibrillation. A mural thrombus and irregular endocardial thickenings—known as MacCallum’s plaques—are evident at their characteristic location. Further InformationThis presentation strongly suggests rheumatic fever, an autoimmune reaction following untreated streptococcal throat infection. It often involves the heart, joints, skin, and brain. Repeated cardiac involvement can lead to chronic rheumatic heart disease, most commonly damaging the mitral valve. Fibrosis causes stenosis, often with characteristic Aschoff nodules and, over time, dilatation of the left atrium. This can trigger atrial fibrillation and mural thrombus formation, ultimately resulting in severe heart failure.

Hypertrophic Subaortic stenosis
Clinical HistoryA 42-year-old American tourist was found dead in his hotel room. A coroner’s autopsy was conducted to investigate the cause of death.PathologyThe heart specimen shows a longitudinal section through both ventricles and the interventricular septum. The most striking feature is the marked thickening of the septum and left ventricular hypertrophy. The aortic and mitral valves appear normal. The enlarged septum narrows the left ventricular lumen. DiagnosisIdiopathic hypertrophic subaortic stenosis, also known as hypertrophic cardiomyopathy. Further InformationSubaortic stenosis is typically acquired, arising from an abnormality in the left ventricular outflow tract (LVOT). Turbulent blood flow in this area may lead to progressive thickening and fibrosis, causing increased resistance and eventual hypertrophy of the left ventricle. While mild cases are often asymptomatic, more advanced disease can present with exertional dyspnoea or syncope. A systolic murmur may suggest the diagnosis, which is typically confirmed via echocardiography. In severe cases, surgical correction of the obstruction is the treatment of choice.

Calcified Aortic Valvular Stenosis Bicuspid Aortic Valve
Clinical HistoryThere is no available clinical history for this specimen.Pathology This specimen is a partial horizontal slice, approximately 1.5 cm thick, taken through the plane of the left atrium. The smooth internal surface of the atrium, the left auricular appendage, and a section of the left ventricle are visible on the inferior aspect. On the superior side, the pulmonary trunk and part of the pulmonary tricuspid valve are visible, along with the aorta and an abnormal bicuspid aortic valve. This valve shows calcified thickening at the opposing margins. Additionally, there is calcification on one of the pulmonary valve cusps. Further InformationA bicuspid aortic valve is the most common congenital heart defect, often undetected until adulthood. It can lead to aortic valve stenosis, which may range from mild to severe. Symptoms—when they occur—include heart murmur, angina, shortness of breath, palpitations, and signs of heart failure such as fatigue and swollen ankles. The narrowed valve forces the left ventricle to work harder, which can lead to ventricular thickening, enlargement, and eventual heart failure. Calcium buildup contributes to valve stiffening, especially in those with bicuspid valves, further narrowing the lumen and restricting blood flow.

Right Ventricular Hypertrophy
Clinical History A 56-year-old woman with emphysema had a two-year history of worsening shortness of breath on exertion and recurrent bronchitis attacks. On examination, her blood pressure was 160/90 mmHg, pulse 96/min, and jugular venous pressure was elevated by 6 cm. The apex beat was impalpable, bilateral lung crepitations were present, and peripheral pitting oedema was noted. ECG showed a right heart strain pattern, and arterial blood gases revealed respiratory acidosis. Despite treatment, her condition steadily deteriorated and resulted in death.Pathology The heart, viewed anteriorly, showed a greatly enlarged and hypertrophied right ventricle. Otherwise, the heart appeared normal. This represents right ventricular hypertrophy (RVH) in a patient with emphysema.Further Information RVH commonly results from chronic lung diseases or structural heart defects. One main cause is pulmonary hypertension (PH), which raises pulmonary artery pressure and leads the right ventricle to compensate by hypertrophy. PH affects about 4 per million people globally, with RVH in approximately 30% of cases. Common causes of PH include chronic obstructive pulmonary disease (COPD), pulmonary embolism, and other restrictive lung diseases. RVH can also be caused by heart defects like tricuspid insufficiency, tetralogy of Fallot, ventricular septal defects, pulmonary valve stenosis, and atrial septal defects. Additionally, RVH is associated with abdominal obesity and elevated systolic blood pressure.

Atrial septal defect
Clinical History A 10-year-old girl with a known congenital heart defect was admitted for surgical repair due to recent onset of cyanosis and cardiac failure. She was breathless, with blood pressure 105/60 mmHg and pulse 140/min. Examination revealed a loud heart murmur at the fourth left intercostal space near the sternum, elevated jugular venous pressure, and bilateral basal lung crepitations but no peripheral oedema. The defect was surgically repaired; however, the patient died following a sudden unexplained post-operative deterioration.Pathology The heart, viewed from the left side, showed a large 3.5 cm ovoid defect in the inter-atrial septum with only a small crescentic rim remaining. The left ventricle was small, while the right ventricle was hypertrophied, demonstrated by a thickened postero-lateral wall. The pulmonary artery was markedly enlarged, with the aortic arch above it and the left auricular appendage nearby.Further Information Atrial septal defect (ASD) is often asymptomatic early in life, even when large. Symptoms arise later due to reversal of the initial left-to-right shunt caused by increasing right ventricular hypertrophy and pulmonary hypertension. This leads to a right-to-left shunt, causing cyanosis, breathlessness, and ultimately congestive heart failure. Types of ASD include: - Secundum: Most common, located in the middle of the atrial septum. - Primum: Lower atrial septum, often with other congenital defects. - Sinus venosus: Rare, upper septum, usually with other heart anomalies. - Coronary sinus: Rare, wall between coronary sinus and left atrium is missing.The exact cause of ASDs is unclear. Some congenital heart defects are familial or linked to genetic conditions like Trisomy 21 (Down’s syndrome). Risk factors during pregnancy include infections (e.g., rubella), substance use (drugs, tobacco, alcohol), exposure to toxins, and maternal conditions such as diabetes or lupus.

Hydatid Disease Affecting the Heart and Aorta
Clinical HistoryAn 11-year-old girl with an 18-month history of hydatid disease underwent three craniotomies to remove 17 brain cysts. Additional cysts were later found in the kidneys, mesentery, and abdominal aorta at its bifurcation. Heart X-ray revealed a calcified cyst, and during its surgical removal, the patient deteriorated and died. A dead hydatid cyst was found in the left ventricle.PathologyThe heart, opened to expose the left ventricle, shows significant left ventricular hypertrophy and an abnormal channel through the posterior mitral valve cusp into the left atrium, surrounded by fibrous tissue. Surgical sutures are visible. The abdominal aorta at the iliac bifurcation is filled with a large antemortem clot. Hydatid cysts are found in both the aortic wall and the ventricular-atrial channel, displaying characteristic layered structures with daughter cysts and surrounding granulomatous reactions.Further InformationHydatid disease is caused by the tapeworm Echinococcus granulosus, transmitted via dog feces. Humans may ingest the eggs, leading to cyst development, most commonly in the liver and lungs. Cardiac involvement is rare (0.5–2% of cases) but can be fatal. Cysts typically form subepicardially and may rarely rupture into the pericardium, causing tamponade or other complications.

Bicuspid Aortic Valve
Clinical History A 64-year-old woman presented with chest pain lasting 5 months, accompanied by breathlessness and wheezing for 4 months. On examination, she was dyspnoeic with an expiratory wheeze, left-sided crepitations, and signs of a right pleural effusion. Pulse and blood pressure were normal. A precordial systolic murmur and a heaving apex beat were noted in the 5th left intercostal space. There was no peripheral oedema. The patient died 4 days after admission.Pathology The heart was opened to reveal the left ventricle and valves. The aortic valve had only two cusps instead of three, with slight patchy thickening but otherwise normal valves. The coronary arteries, including the left circumflex artery, were widely patent. Dense pericardial fibrosis and adhesions on the posterior heart surface indicated constrictive pericarditis. Autopsy also showed ascites, a small cirrhotic liver, bilateral pleural effusions, and right lung collapse. Death was due to liver cirrhosis and failure, possibly linked to the pericarditis. The bicuspid aortic valve was an incidental finding.Further Information Bicuspid aortic valve is a common congenital anomaly, often asymptomatic until later in life. It predisposes to calcific aortic stenosis, usually in the 5th to 7th decades. The valve may be isolated or part of syndromes such as Tetralogy of Fallot. Fusion of two cusps results in unequal leaflet sizes, causing abnormal valve motion and turbulence, which increase the risk of aortic dilation, dissection, and calcification. Over time, this can lead to aortic stenosis or regurgitation, with symptoms like dyspnoea and reduced exercise tolerance. Diagnosis is confirmed by transthoracic echocardiography.

Tetralogy of Fallot
Clinical HistoryA 21-month-old boy presented with a 2–3 month history of exhaustion and exertional dyspnoea. He had experienced several short episodes of acute breathing difficulty. On admission, he showed central cyanosis, mild finger clubbing and a harsh systolic murmur at the left sternal edge. Cardiac catheterisation confirmed Tetralogy of Fallot and severe pulmonary oedema. A Willis-Potts surgical anastomosis was performed. Unfortunately, the child died 12 hours post-operatively following acute dyspnoea and left lung consolidation.PathologyThe heart, viewed anteriorly, shows right ventricular hypertrophy and pulmonary outflow tract narrowing. The pulmonary valve is bicuspid and stenosed with visible endocardial fibrosis below. The aorta overrides a large ventricular septal defect (VSD) and communicates with the hypertrophied right ventricle. A probe inserted through the narrowed pulmonary trunk reaches the dilated left pulmonary artery and continues through the surgical anastomosis into the descending aorta. Posteriorly, the opened heart reveals a large atrial septal defect (ASD) and a second smaller ASD. Notably, the left ventricular wall is thinner than the right. Further InformationTetralogy of Fallot includes four key defects: 1. Ventricular septal defect, 2. Overriding aorta communicating with both ventricles, 3. Pulmonary stenosis, and 4. Right ventricular hypertrophy. Cyanosis typically appears early and its severity depends on the degree of right ventricular outflow obstruction. Some patients may survive untreated into adulthood, though surgical correction is now standard. Additional defects such as ASD may coexist. While the exact cause is unknown in many cases, genetic links include Down syndrome and DiGeorge syndrome.

Continuous innovation

Social responsibility

Active customer orientation

Understanding quality

Sustainable actions

ISO 9001 certification