

















Product information "Ventriculitis, Secondary to Septicaemia"
Clinical History
A 50-year-old male with alcoholism was admitted with a 2-week history of weakness and shortness of breath. He initially presented with productive cough, chest pain, and blood-stained sputum. On examination, he was febrile, cyanosed, and drowsy, with grunting respiration and a friction rub over the right lower lobe. His condition worsened progressively. Shortly before death, a lumbar puncture yielded green opalescent fluid. Blood cultures confirmed Streptococcus pneumoniae.
Pathology
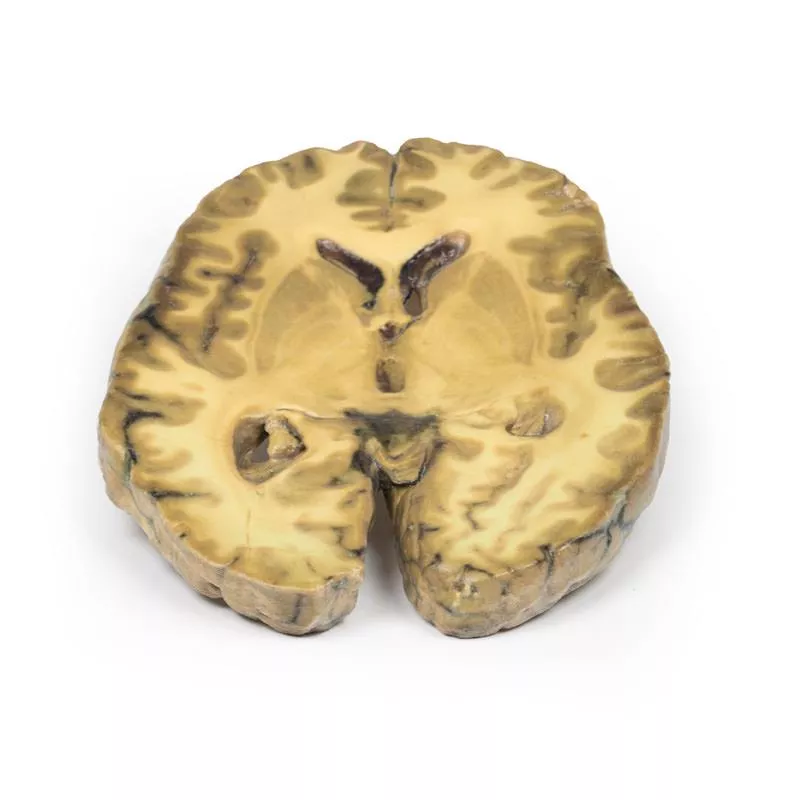
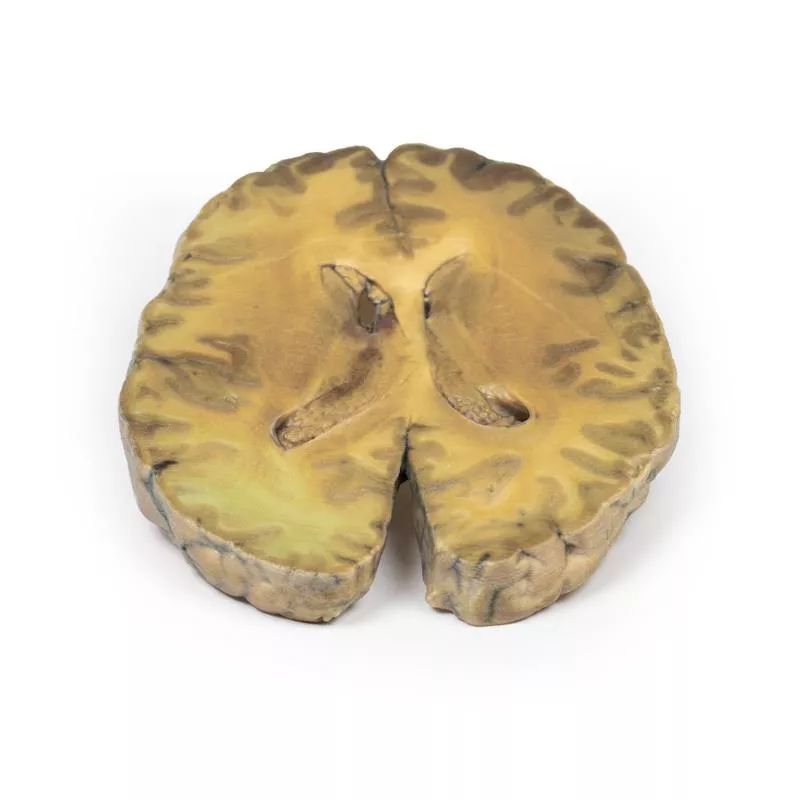
This is a case of ventriculitis, alongside pneumococcal meningitis and right basal pneumonia. A horizontal brain section shows both lateral ventricles with a thickened, rough ependymal lining and cellular debris near the choroid plexus and anterior horn. Structures like the caudate nucleus, lentiform nucleus and internal capsule are visible. Histology revealed extensive neutrophilic infiltration of the subarachnoid space, vascular wall involvement, and cerebral parenchymal inflammation causing haemorrhage and necrosis.
Further Information
Ventriculitis is a rare complication of intracranial infection. In adults, it usually occurs secondarily to surgery or trauma rather than primary meningitis. Common pathogens include staphylococci and resistant Gram-negative bacilli. In infants under 6 months, incidence is higher. Symptoms may mimic hydrocephalus due to aqueductal obstruction. Diagnosis relies on CSF analysis and imaging (CT, MRI). Treatment involves prolonged intravenous antibiotics that can penetrate CSF and brain tissue.
A 50-year-old male with alcoholism was admitted with a 2-week history of weakness and shortness of breath. He initially presented with productive cough, chest pain, and blood-stained sputum. On examination, he was febrile, cyanosed, and drowsy, with grunting respiration and a friction rub over the right lower lobe. His condition worsened progressively. Shortly before death, a lumbar puncture yielded green opalescent fluid. Blood cultures confirmed Streptococcus pneumoniae.
Pathology
This is a case of ventriculitis, alongside pneumococcal meningitis and right basal pneumonia. A horizontal brain section shows both lateral ventricles with a thickened, rough ependymal lining and cellular debris near the choroid plexus and anterior horn. Structures like the caudate nucleus, lentiform nucleus and internal capsule are visible. Histology revealed extensive neutrophilic infiltration of the subarachnoid space, vascular wall involvement, and cerebral parenchymal inflammation causing haemorrhage and necrosis.
Further Information
Ventriculitis is a rare complication of intracranial infection. In adults, it usually occurs secondarily to surgery or trauma rather than primary meningitis. Common pathogens include staphylococci and resistant Gram-negative bacilli. In infants under 6 months, incidence is higher. Symptoms may mimic hydrocephalus due to aqueductal obstruction. Diagnosis relies on CSF analysis and imaging (CT, MRI). Treatment involves prolonged intravenous antibiotics that can penetrate CSF and brain tissue.
Login
Erler-Zimmer
Erler-Zimmer Medical GmbH
Hauptstrasse 27
77886 Lauf
Germany
info@erler-zimmer.de
Achtung! Medizinisches Ausbildungsmaterial, kein Spielzeug. Nicht geeignet für Personen unter 14 Jahren.
Attention! Medical training material, not a toy. Not suitable for persons under 14 years of age.
Other customers also bought

Berry Aneurism of Basilar Artery
Clinical HistoryA 37-year-old patient presented with headache, vomiting, and disorientation after head trauma. CT revealed dilated lateral ventricles and a mass projecting into the third ventricle. A shunt was placed for hydrocephalus. Angiography identified a partially thrombosed 1 × 1 cm basilar artery aneurysm. The aneurysm enlarged over time, and multiple surgical attempts, including ligation and shunt revisions, were unsuccessful. The patient remained unconscious and later died.PathologyThis mid-sagittal brain section (1 cm thick) shows a large, dark berry aneurysm (5 × 2 cm) from the basilar artery, eroding into the midbrain and pons, and compressing the third ventricle. The aneurysm is filled with a laminated thrombus, with blood visible in the third ventricle and signs of leakage. A mucoid degeneration (0.4 cm) is present in the pons. The lateral view shows ventricular dilatation, blood staining, and haemorrhagic infarction of the caudate nucleus, along with meningeal discolouration consistent with subarachnoid haemorrhage. Further InformationIntracranial aneurysms occur in ~3.2% of the population, with rupture rates of 7.9 per 100,000 person-years. Posterior circulation aneurysms are less common and typically found at basilar, vertebral, or cerebellar artery junctions. Symptoms arise from subarachnoid haemorrhage or mass effect. Complications include raised intracranial pressure, hydrocephalus, re-bleeding, and vasospasm. Treatment options include surgical and endovascular interventions.

Metastatic Adenocarcinoma in the Brain
Clinical HistoryA 56-year-old male underwent a total gastrectomy and splenectomy for gastric adenocarcinoma. Over two months, he developed a progressively unsteady gait, left hand weakness, and frontal headaches with nausea and vomiting. Imaging revealed a right frontal lobe lesion. Following craniotomy and resection, pathology confirmed a metastatic gastric adenocarcinoma. The patient's condition worsened with jaundice, papilloedema, and declining consciousness due to increased intracranial pressure. Repeat imaging showed recurrence of the brain lesion and liver metastases. He died 9 months after gastrectomy.PathologyThis coronal brain section reveals a well-defined, variegated pink-grey tumour in the right frontal lobe, involving both grey and white matter. There is visible compression of the right lateral ventricle and midline shift caused by the mass. Further InformationStomach cancer is a leading cause of cancer-related death worldwide. Risk factors include male sex, diet, smoking, and Helicobacter pylori infection. Gastric adenocarcinoma most commonly metastasises to the liver, peritoneum, lungs, and bones. Brain metastases are rare (weniger als 1 %) and typically occur in widespread disease, carrying a poor prognosis. Palliative care may include surgery, radiotherapy, steroids, chemotherapy, or combinations thereof.

Left cerebral infarct
Clinical HistoryThe patient was a 51-year-old woman who had suffered a cerebrovascular accident two years before death, resulting in left-sided hemiplegia. At autopsy, she showed severe generalised atherosclerosis and an old myocardial infarction in the left ventricle with an overlying mural thrombus.PathologyA coronal section of the brain reveals irregular cystic cavities in the region supplied by the right middle cerebral artery, consistent with an old infarct. The cavity walls are yellow and partially collapsed. There is compensatory dilatation of the left lateral ventricle. The arteries below the mammillary bodies appear moderately atheromatous, though this is not easily seen macroscopically. Further InformationGiven the history of cardiac disease and a mural thrombus, the cerebral infarct was most likely caused by a thromboembolus originating from the heart.

Meningioma
Clinical HistoryA 68-year-old woman presented with new-onset seizures and was diagnosed with epilepsy. A collateral history revealed a gradual personality change. Several months later, she died from a myocardial infarction.PathologyThe tumour is located between the two frontal lobes, compressing them. It has a pinkish cut surface with yellow areas indicating necrosis and is attached anteriorly to the dura mater. This represents a typical meningioma. Further InformationMeningiomas are among the most common tumours associated with the central nervous system, though they originate from the arachnoid cells of the meninges (not the CNS itself). They are often attached to the dura or its folds (e.g. falx cerebri, tentorium cerebelli) and are typically slow-growing and benign.Symptoms depend on tumour size and location and may include seizures, personality changes, sensory disturbances, or signs of increased intracranial pressure. Many meningiomas remain asymptomatic.Treatment ranges from depending on clinical presentation and tumour type.Meningiomas are rare in children. The median age at diagnosis is 65, and they are more common in women (3:2). Ionising radiation, especially cranial radiotherapy, increases the risk. The strongest genetic predisposition is seen in neurofibromatosis type 2 (NF2), a dominant disorder caused by NF2 gene mutations on chromosome 22, often resulting in multiple nervous system tumours.

Glioma grade 3-4, causing papilloedema
Clinical HistoryThe patient was a 24-year-old woman who initially presented with an abnormal EEG following a single epileptic seizure. Six months later, she developed blurred vision and headaches. Ophthalmoscopy revealed bilateral papilloedema, though no focal neurological signs were found. Imaging identified a space-occupying mass, biopsied and diagnosed as a Grade III–IV glioma. She underwent radiotherapy, but a month later developed weakness in her left arm and leg. Shortly thereafter, she was admitted with drowsiness and vomiting and died soon after.PathologyThe specimen reveals a large intracerebral tumour, obliterating the lateral ventricles and the inner two-thirds of the internal capsule and basal ganglia on the right. The tumour crosses the corpus callosum and distorts the aqueduct. It is relatively well-demarcated and highly vascular, with extensive haemorrhage and necrosis, giving it a mottled appearance.

Cerebral Haemorrhage, secondary to Acute Myeloid Leukaemia
Clinical HistoryA 22-year-old male presented with a two-week history of malaise, weight loss and unexplained bruising. He later developed productive cough and fever. Shortly after hospital admission for further tests, he suddenly lost consciousness and died within minutes.PathologyThis horizontal brain section shows the superior surface with two large haemorrhages in the right frontal and parietal lobes (each approx. 5 cm), as well as multiple smaller haemorrhages in the white matter bilaterally. This presentation is consistent with multiple intraparenchymal haemorrhages in a patient with acute myeloid leukaemia (AML). Further InformationIntraparenchymal brain haemorrhages result from rupture of small blood vessels in the brain and often present with sudden neurological decline. In AML, bone marrow failure due to immature blast accumulation leads to thrombocytopaenia, increasing the risk of spontaneous bleeding. Intracranial haemorrhage is the second most common cause of death in AML after infection. A severe bleeding disorder, disseminated intravascular coagulation (DIC), can also occur. Treatment options depend on the severity and may include haematoma evacuation, seizure control and management of intracranial pressure. Mortality for intracerebral haemorrhage is high, especially within the first 48 hours.

Cerebral Haemorrhage
Clinical HistoryA 56-year-old woman was admitted after two episodes of severe headache accompanied by loss of consciousness. Examination revealed systemic hypertension, cardiac enlargement, and right-sided hemiparesis. Angiography detected bilateral middle cerebral artery aneurysms. Her condition rapidly worsened, and she died shortly after admission.PathologyThe left cerebral hemisphere, sectioned parasagittally, shows a large cerebral haemorrhage involving the parietal and frontal lobes. The haemorrhage and associated clot have significantly distorted the external capsule and lateral ventricle. The bleeding originated from a ruptured aneurysm of the left middle cerebral artery.

Pituitary Adenoma
Clinical HistoryA 29-year-old male presented with a 22-month history of headaches and blurred vision. Examination revealed a bitemporal hemianopia and a left sixth nerve palsy. Skull X-ray showed erosion of the sphenoid body, with some of the dorsum sellae and anterior clinoid process intact. Carotid angiography demonstrated upward and lateral displacement of the anterior and middle cerebral arteries. Pneumoencephalography showed upward displacement of the lateral and third ventricles. A craniotomy was performed, but the patient died immediately after surgery.PathologyThe pituitary gland has been completely replaced by a 4 cm round tumour, seen in a sagittal brain section to the right of the falx cerebri. The cut surface of the tumour is pale brown and homogeneous, with a small area of haemorrhage likely caused by surgical trauma. The tumour caused upward displacement of the midbrain and erosion of the sphenoid bone, enlarging the sella turcica. The optic chiasma is compressed. Histological diagnosis: chromophobe adenoma of the anterior pituitary. Further InformationThis case used now outdated methods such as pneumoencephalography. Today, a CT followed by a brain MRI would be standard. Pituitary adenomas are the most common pituitary tumours, typically affecting adults between 35 and 60 years. Clinical signs relate to mass effect—including increased intracranial pressure, bony erosion, and optic chiasma compression—as well as hormonal activity. About 75% are functioning adenomas (e.g., prolactin, growth hormone, or ACTH secretion), while non-functioning tumours may present later and cause hypopituitarism due to compression of the remaining gland.

Continuous innovation

Social responsibility

Active customer orientation

Understanding quality

Sustainable actions

ISO 9001 certification