

















Product information "Glioblastoma multiforme"
Clinical History
Over a 3-year period, a 57-year-old woman experienced intermittent frontal headaches and memory disturbances that progressed to psychiatric symptoms, vomiting, and meningeal signs. Localising neurological signs appeared only late in the disease course.
Pathology
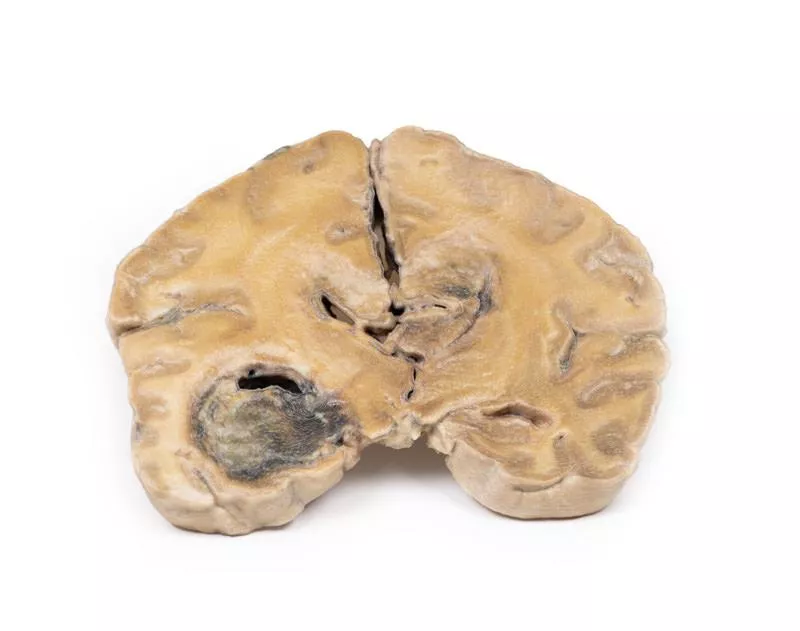
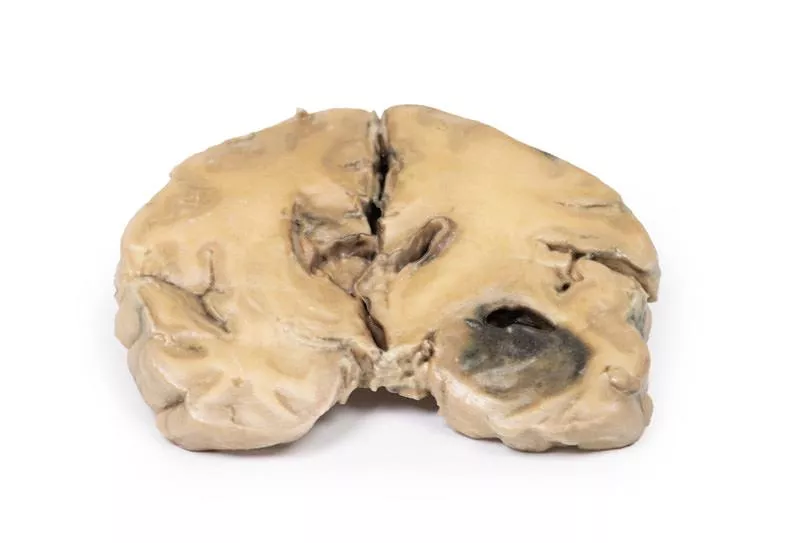
A coronal section of the cerebral hemisphere reveals a round, haemorrhagic, variegated tumour in the left temporal lobe. Tumour tissue extends across the midline, replacing the corpus callosum and nearly obliterating the ventricular system. Further sections confirmed these lesions are part of one massive tumour.
Further Information
Gliomas are the second most common CNS cancer after meningiomas. These tumours resemble normal macroglial cells—astrocytes, oligodendrocytes, and ependymal cells—and arise from progenitor cells differentiating along these lines. Glioblastoma multiforme (GBM), a grade IV astrocytoma, can develop de novo or from lower-grade gliomas. Histologically, GBMs feature necrosis surrounded by anaplastic cells and hyperplastic blood vessels. GBMs are more frequent in males and typically diagnosed in the 6th decade. Risk factors include neurofibromatosis type 1, Li-Fraumeni syndrome, and prior brain radiotherapy. Symptoms depend on tumour location and include persistent headaches, visual disturbances, vomiting, appetite loss, mood and personality changes, cognitive decline, new seizures, and speech difficulties. Diagnosis relies on CT and MRI. About 50% of GBMs involve more than one hemisphere and often invade ventricular walls or meninges, occasionally reaching the CSF. Metastases outside the CNS are rare. Tumour growth causes cerebral oedema and increased intracranial pressure. These aggressive tumours have a median survival of around 3 months if untreated. Treatment includes surgery, radiation, and chemotherapy.
Over a 3-year period, a 57-year-old woman experienced intermittent frontal headaches and memory disturbances that progressed to psychiatric symptoms, vomiting, and meningeal signs. Localising neurological signs appeared only late in the disease course.
Pathology
A coronal section of the cerebral hemisphere reveals a round, haemorrhagic, variegated tumour in the left temporal lobe. Tumour tissue extends across the midline, replacing the corpus callosum and nearly obliterating the ventricular system. Further sections confirmed these lesions are part of one massive tumour.
Further Information
Gliomas are the second most common CNS cancer after meningiomas. These tumours resemble normal macroglial cells—astrocytes, oligodendrocytes, and ependymal cells—and arise from progenitor cells differentiating along these lines. Glioblastoma multiforme (GBM), a grade IV astrocytoma, can develop de novo or from lower-grade gliomas. Histologically, GBMs feature necrosis surrounded by anaplastic cells and hyperplastic blood vessels. GBMs are more frequent in males and typically diagnosed in the 6th decade. Risk factors include neurofibromatosis type 1, Li-Fraumeni syndrome, and prior brain radiotherapy. Symptoms depend on tumour location and include persistent headaches, visual disturbances, vomiting, appetite loss, mood and personality changes, cognitive decline, new seizures, and speech difficulties. Diagnosis relies on CT and MRI. About 50% of GBMs involve more than one hemisphere and often invade ventricular walls or meninges, occasionally reaching the CSF. Metastases outside the CNS are rare. Tumour growth causes cerebral oedema and increased intracranial pressure. These aggressive tumours have a median survival of around 3 months if untreated. Treatment includes surgery, radiation, and chemotherapy.
Login
Erler-Zimmer
Erler-Zimmer Medical GmbH
Hauptstrasse 27
77886 Lauf
Germany
info@erler-zimmer.de
Achtung! Medizinisches Ausbildungsmaterial, kein Spielzeug. Nicht geeignet für Personen unter 14 Jahren.
Attention! Medical training material, not a toy. Not suitable for persons under 14 years of age.
Other customers also bought

Intracranial space-occupying lesion
Clinical HistoryA 56-year-old woman with a 6-month history of intermittent headaches and vomiting was admitted to hospital in a comatose state following a grand mal seizure. She did not regain consciousness.Pathology This coronal brain section reveals that the brain has been compressed laterally and downward due to a large intracranial mass on the right side, likely a meningioma (though the tumour itself is not present in the section). The anterior view shows a midline shift with subfalcine herniation of the cingulate gyrus. The posterior view displays haemorrhages of varying ages in the temporal lobe and pons, which are typical for a supratentorial mass lesion. There is also noticeable ventricular asymmetry. Further Information A space-occupying meningioma can exert pressure on brain tissue, resulting in atrophy and displacement, which in turn may affect cranial nerve function, blood flow, and normal brain processes. Common symptoms may include: - Seizures – such as myoclonic (brief muscle jerks or spasms) or tonic-clonic (loss of consciousness, muscle rigidity, followed by convulsions and potential loss of body control). - Sensory disturbances – changes in vision, smell, or hearing without loss of consciousness.The presentation can vary depending on the tumour’s location.

Astrocytoma
Clinical HistoryA 73-year-old woman was admitted with new left-sided hemiplegia. On further questioning, she reported a 3-month history of headaches, nausea, and worsening balance. CT identified an inoperable brain tumour. She passed away one week after admission.Pathology A coronal brain slice reveals a poorly demarcated tumour in the right temporal lobe, causing hemispheric enlargement and flattening of the gyri. The posterior view shows subfalcine herniation, and the mass displays areas of necrosis and haemorrhage. Histology confirmed an astrocytoma, Grade III/IV. Further InformationAstrocytomas are a subtype of glioma, the second most common CNS cancer after meningioma. Originating from astrocytes, they are classified by grade—diffuse (II), anaplastic (III), to glioblastoma (IV). Typical histology shows gemistocytes with eosinophilic cytoplasm against a fibrillary background. Most occur in the hemispheres of patients aged 40–60 and present with seizures, headaches, nausea, or focal deficits. Without treatment, median survival for Grade III tumors is ~~18 months. Management involves surgery, radiotherapy, chemotherapy, or combinations tailored to the patient.

Metastatic carcinoma in the brain
Clinical HistoryThis 51-year-old woman had undergone surgery for breast carcinoma two years before presenting with left-sided ataxia of two weeks’ duration. A previous fainting episode followed by weakness on the same side had preceded this. Examination revealed left spastic paresis. Due to the rapid onset of symptoms, a vascular lesion was suspected. Despite discharge, she was re-admitted six weeks later with left-sided seizures. Lumbar puncture and clinical re-evaluation were inconclusive, but EEG showed a right anterior temporal abnormality. Angiography then revealed a large space-occupying lesion in the right cerebrum. Her condition continued to deteriorate, ultimately resulting in death.PathologyThe horizontal brain slice reveals three cystic tumours, predominantly in the right parietal region. The largest measures 5 cm in diameter. Another tumour is seen near its posterior margin, and a third, smaller one is found in the left parietal region. The tumours mainly affect the white matter, with shaggy, friable greyish tissue walls. The largest tumour had ulcerated into the right lateral ventricle, and subfalcine herniation with displacement of the basal ganglia and internal capsule was observed. Histology confirmed metastatic carcinoma. Additional metastases were found in the liver and bone, consistent with a primary breast carcinoma.

Glioblastoma multiforme
Clinical HistoryA 56-year-old male presented with a generalised seizure after which he remained unconscious and later died. A history revealed 6 months of progressive confusion, short-term memory loss, and personality changes.PathologyPost-mortem coronal brain sections show a 4 cm necrotic and haemorrhagic tumour invading from the inferior frontal lobe into the lateral ventricle. Meningeal spread is visible on the posterior aspect. Further InformationGliomas are the second most common central nervous system cancers after meningiomas. They originate from glial-like cells such as astrocytes, oligodendrocytes, or ependymal cells. Glioblastoma multiforme (GBM), a grade IV astrocytoma, arises from astrocytes and may develop de novo or from lower-grade tumours. GBMs typically show necrosis surrounded by anaplastic cells and hyperplastic blood vessels. More frequent in males, GBM commonly occurs in the 6th decade. Risk factors include neurofibromatosis type 1, Li-Fraumeni syndrome, and prior brain radiotherapy. Symptoms depend on tumour location and include persistent headaches, visual disturbances, vomiting, appetite loss, mood and personality changes, cognitive decline, seizures, and speech difficulties. Diagnostic tools are CT and MRI. About 50% of GBMs involve more than one hemisphere, often invading ventricles or meninges, with rare spinal cord spread. Metastasis outside the CNS is uncommon. Tumour growth leads to cerebral oedema and increased intracranial pressure. These aggressive tumours have a median survival of approximately 3 months if untreated. Treatment consists of surgery followed by radiation and chemotherapy.

Metastatic melanoma
Clinical HistoryIn the 1970s, a 31-year-old woman presented with severe headache and diplopia, eight months after the removal of an invasive pigmented skin melanoma from her neck. Initial clinical examination revealed no abnormalities. She was discharged but re-admitted later with persistent vomiting. Her condition rapidly deteriorated, and she died shortly after.PathologyThe brain specimen shows extensive intracerebral melanoma metastases. The inferior surface displays numerous dark nodules up to 1.5 cm in diameter. On the cut superior surface, similar lesions are visible and confined to the grey matter. The tumour nodules are not encapsulated and infiltrate the cortex, with areas of necrosis and haemorrhage present. Further InformationMelanoma accounts for about 10% of all brain metastases. Risk increases with age over 60, male gender, disease progression, and certain genetic mutations such as BRAF or NRAS. Most metastases are supratentorial and may present with headache, neurological deficits or seizures. These lesions have a known risk of spontaneous haemorrhage. Diagnosis is based on imaging and histological confirmation. Treatment often involves stereotactic radiosurgery, radiotherapy, and systemic immunotherapy or targeted therapies, improving median survival to around 11 months in recent years.

Ruptured Berry Aneurysm
Clinical History A 38-year-old woman developed sudden pain behind the right eye, followed by progressive weakness of the left leg. On examination, she was confused and hypertensive with left-sided hemiparesis, right homonymous hemianopia, and a right VIth cranial nerve palsy. Reflexes were brisk on the left side, with an upgoing plantar reflex. Lumbar puncture revealed raised pressure and blood-stained CSF. Angiography identified an intracerebral aneurysm, which was clipped surgically. Unfortunately, the patient died suddenly the day after surgery.Pathology The basal brain surface shows a 5 mm saccular aneurysm at the junction of the right internal carotid and posterior communicating artery, which had ruptured. Subarachnoid haemorrhage is visible in the cisterna magna and on the inferior right frontal lobe. A similar unruptured aneurysm is also present on the left. The right frontal lobe appears soft and friable. Further Information Posterior communicating artery aneurysms are the third most common among Circle of Willis aneurysms and can compress nearby cranial nerves, such as the abducens (VI). The patient’s retro-orbital pain may relate to irritation of the trigeminal nerve, while the visual field defect likely resulted from pressure on the right optic tract. Neurological symptoms depend on the affected vascular territory of the cerebral cortex.

Cerebral Arterio-Venous Malformation
Clinical HistoryThis 58-year-old patient died due to post-operative complications following transurethral resection of the prostate. He had experienced two episodes of transient neurological deficits at the ages of 28 and 35. At 50, he developed a permanent hemiparesis affecting the left leg, primarily the ankle.PathologyThis coronal brain slice through the parietal lobes reveals a 4 cm lesion in the medial right hemisphere, extending from the cortical surface to the lateral ventricle. The abnormal area consists of tortuous vascular channels and interspersed tissue. Histology confirmed an arteriovenous malformation (AVM) with glial tissue surrounding vessels of both arterial and venous character. Further InformationCerebral AVMs can cause a range of symptoms such as headaches, seizures, and cranial nerve deficits, though some patients remain asymptomatic. In serious cases, vessel rupture may lead to intracranial haemorrhage, resulting in loss of consciousness, nausea, vomiting, and vision problems. Neurological deficits like hemiparesis or aphasia may occur depending on the bleed location. Ruptured AVMs carry significant risks of both mortality and long-term disability.

Craniopharyngioma
Clinical HistoryA 62-year-old woman presented with disorientation to time, place, and person. Physical examination showed no localized neurological deficits. Imaging revealed a space-occupying lesion in the floor of the 3rd ventricle. During surgery, tissue was removed but complete excision was not possible. Histology confirmed the diagnosis of Craniopharyngioma. Postoperatively, the patient developed complex metabolic disturbances likely originating from the hypothalamus. Her condition worsened gradually, and she died 10 weeks after admission following gastric aspiration.PathologyThe sagittally sectioned brain shows a pink-grey, ovoid tumour measuring 2.5 x 1.5 cm located in the hypothalamic region. The tumour is encapsulated except at the ventral pole where surgery had removed tissue. The cut surface reveals a microcystic or spongy appearance. It distorts the 3rd ventricle and blocks the Foramen of Munro. The optic chiasm is displaced downward. A previous ventriculo-atrial shunt prevented dilation of the lateral ventricles despite this obstruction. Further InformationCraniopharyngiomas account for 1-3% of all brain tumours and 5-10% in children, with two age peaks: 5-14 years and 50-75 years. Higher incidence is reported in Japan and parts of Africa. These epithelial tumours arise mainly from the pituitary stalk but can also originate in the sella turcica, optic system, or third ventricle. They often have both solid and cystic components, the cysts containing cholesterol crystals. Two main types exist: adamantinomatous and papillary, differing in histology and genetics though prognostic relevance remains unclear. Treatment involves surgical resection and radiation therapy to address residual disease. Prognosis depends on tumour control and complications from local and endocrine effects.

Intracerebral Haemorrhage
Clinical HistoryAn 80-year-old man suddenly lost consciousness. On examination, there was a right gaze palsy, left hemiplegia, and right hemiparesis.Pathology Coronal sections at the level of the mammillary bodies, including the brainstem and anterior temporal lobes, show a massive clot replacing tissue in the left basal ganglia and internal capsule. The haemorrhage ruptured into the left lateral ventricle and temporal horn, destroying its walls and infiltrating adjacent brain. The right lateral ventricle is also filled with blood but retains intact walls. The clot acts as a space-occupying lesion, expanding the left hemisphere and shifting midline structures rightward. A subfalcine herniation of the left cingulate gyrus under the falx cerebri is evident. Further Information Intracerebral haemorrhages of this type commonly result from systemic hypertension. The bleed arises from the rupture of a micro-aneurysm in striate artery branches supplying the basal ganglia.

Continuous innovation

Social responsibility

Active customer orientation

Understanding quality

Sustainable actions

ISO 9001 certification